Indications
- Symptoms of cardiac tamponade such as Beck’s triad1:
- Jugular venous distention
- Distant heart sounds
- Hypotension
- Other signs
- Pulsus paradoxus greater than 10 mmHg
- Low voltage QRS
- Electrical alternans
- Enlarged cardiac silhouette
- Dyspnoea and tachycardia are the most common symptoms experienced
- Symptom burden is dependent on the acuity of pericardial effusion build up
- Risk factors
- Metastatic cancer
- History of mediastinal radiation
- End-stage renal disease
- Tuberculosis
- Traumatic injury
- Recent cardiac surgery
Contraindication
- Relative
- A relative contraindication exists for traumatic pericardial effusion with unstable vital signs as this is an indication for an emergency thoracotomy; there will be rapid re-accumulation of blood within the pericardium
- Myocardial rupture
- Aortic dissection
- Severe bleeding disorder
- Nil absolute contraindications
Complications
- Cardiac dysrhythmias
- Cardiac puncture
- Pneumothorax
- Coronary vessel injury
- Peritoneal puncture
- Liver or stomach injury
- Puncture of the internal thoracic artery
- Diaphragmatic injury
Equipment
- Code cart and resuscitation equipment
- Haemodynamic monitoring
- Echocardiogram/ultrasound
- ECG monitoring
- 18-gauge spinal needle
- Three-way tap
- 20 mL syringe
- Anti-bacterial skin cleanser
- Wire with alligator clips
- Sterile gloves and gown
- Local anaesthetic if permissable
Method
- Palpate surface landmarks for the xiphoid process
- Clean area with anti-bacterial skin cleanser
- Drape the area
- Use local anaesthetic if time permits
Sub-Xiphoid Approach
- Consider raising the head by 30-45 degrees
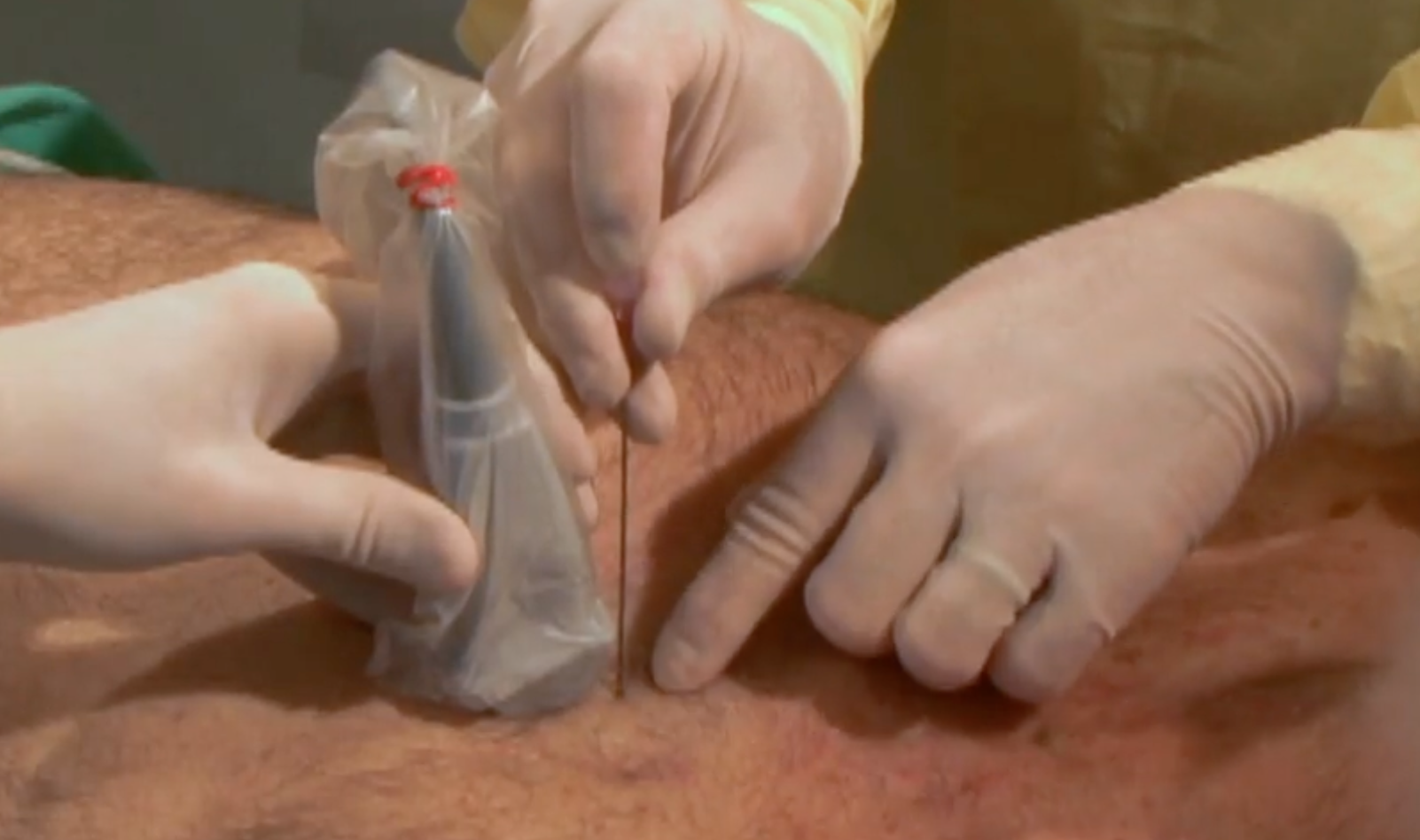
- Insert the spinal needle with the stylet in place using the subxiphoid approach and an ultrasound as guidance
- Remove the stylet once entered the skin/dermal tissue and connect the three way stop clock and a 2 mL syringe
- Advance the needle towards the left shoulder while aspirating continuously
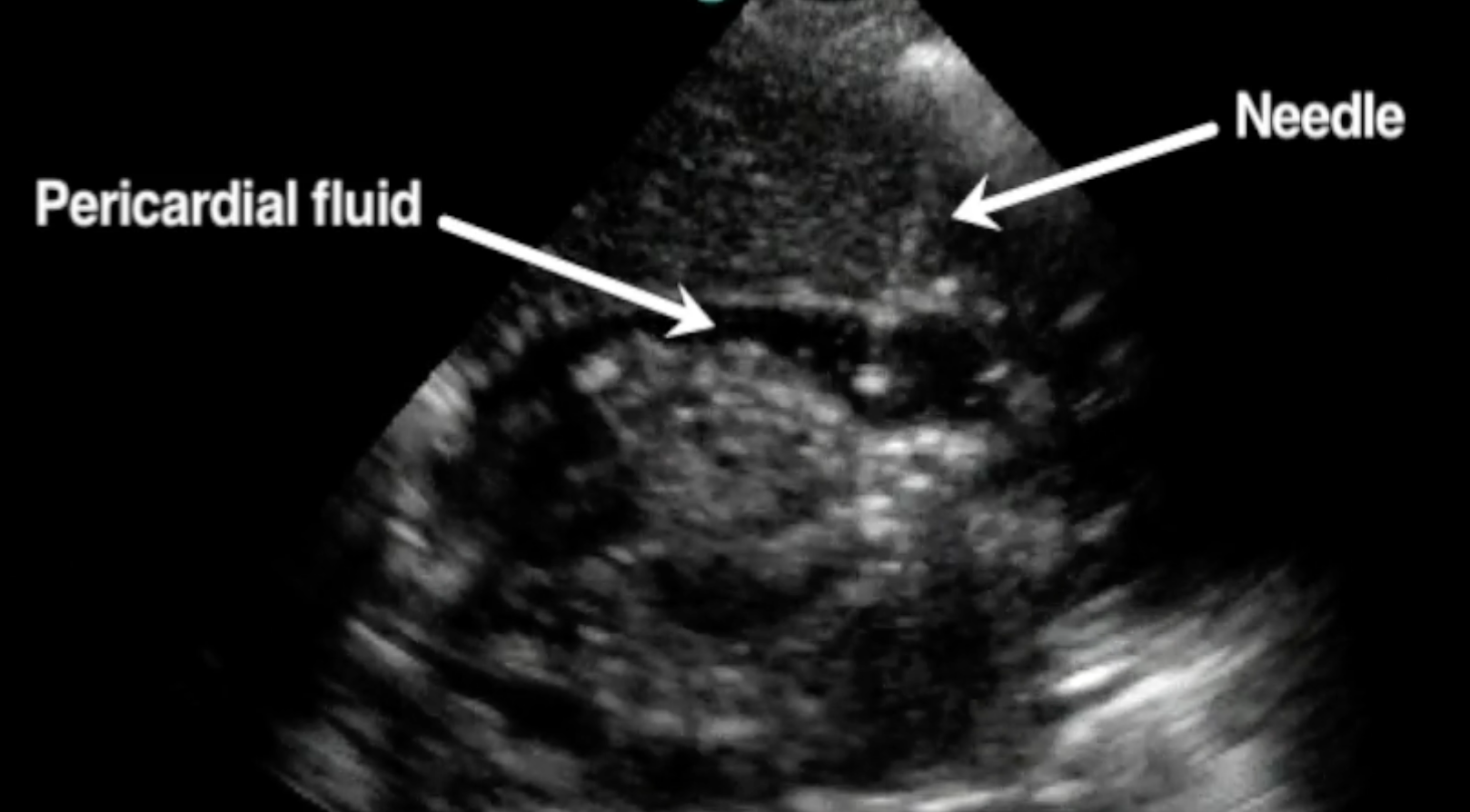
- Withdraw fluid from the pericardial effusion
- Once happy, attach tubing to a three-way stop clock to allow further removal
Parasternal Approach
- Similarly insert the needle but use a perpendicular approach at the 5th intercostal space just lateral to the sternum using an ultrasound to find the largest area of collection
- Remove the stylet on entering the skin
- Attach three way needle and 20 mL syringe
Electrocardiographic Monitoring
- Connect the spinal needle to a precordial lead using the aligator clips

- Monitor for ST elevation in associated lead while advancing the needle which indicates advancement of the needle too far
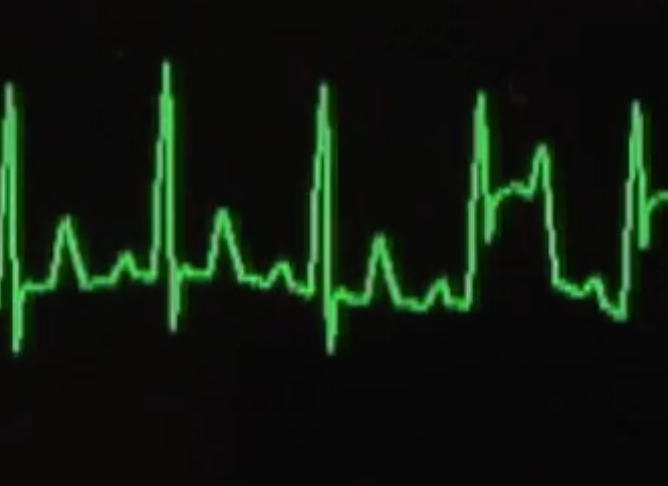
- Withdraw the needle until ST-elevation resolves and re-direct the needle for pericardiocentesis
Aftercare
- Obtain ultrasound and chest X-ray to assess for complications such as pleural effusion and pneumothorax
- Ongoing monitoring
Sources
- Fitch, M.T., McGinnis, H.D., 2012. Emergency Pericardiocentesis. n engl j med.
- Pericardiocentesis in cardiac tamponade: indications and practical aspects
Footnotes
-
Note that all signs rarely appear together and when they do indicate a patient is peri-arrest ↩