Pressure
- Hydrostatic pressure is the pressure present in a fluid at rest due to gravity
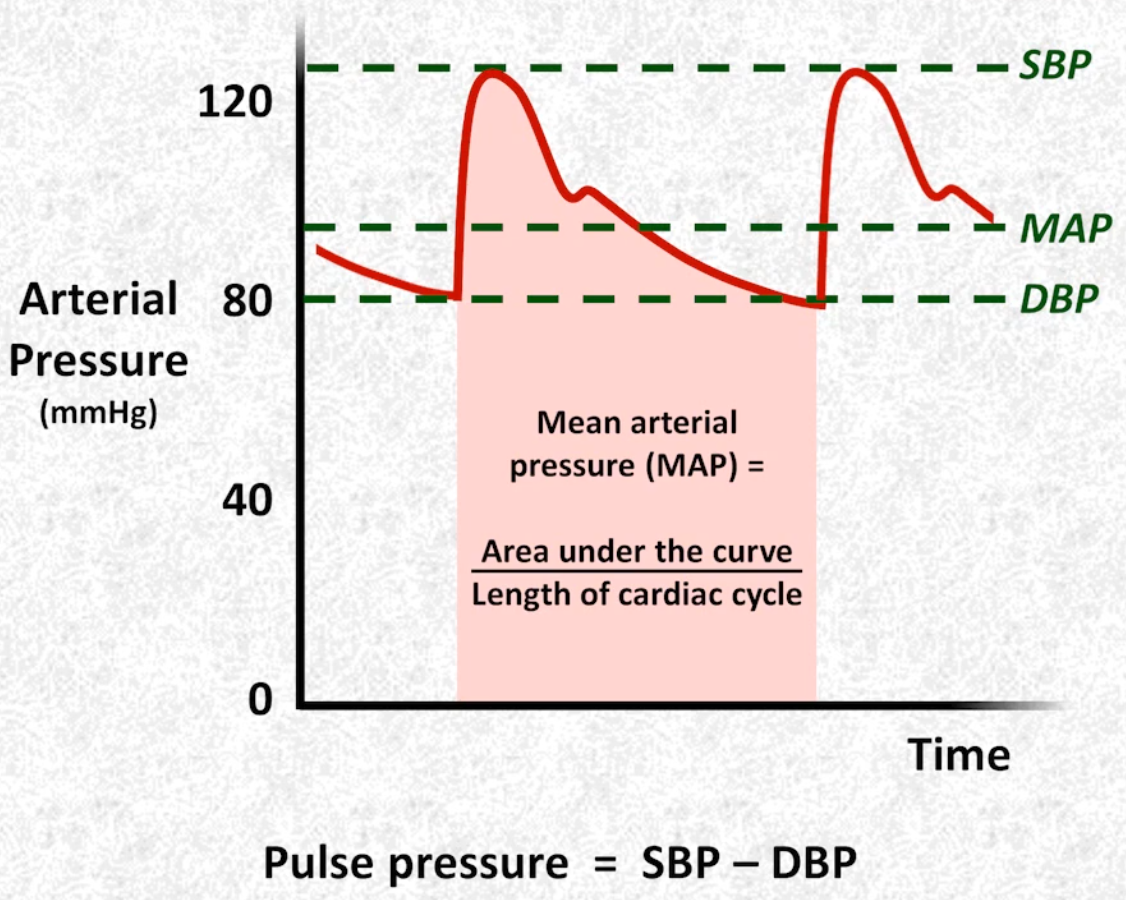
- Mean arterial pressure is the area under the pressure time curve divided by the length of the cardiac cycle
- It can be estimated by the following equations:
- Determinants of SBP
- Arterial compliance
- Stroke volume
- Systemic vascular resistance
- Determinants of DBP
- Systemic vascular resistance
- Arterial compliance
- Heart rate
- Determinants of pulse pressure:
Preload
- Defined as either:
- Wall tension experienced by the LV at end-diastole (estimated by LV end-diastolic pressure)
- Sarcomere length in the LV at end-diastole (estimated by LV end-diastolic volume)
- It is influenced by:
- Total blood volume
- Ventricular compliance
- Wall thickness
- Relaxation (lusitropic) properties
- Pericardial compliance
- Rhythm
- Heart rhythm (as heart rate increases, less time is spent in diastole)
- Arrythmias where there is no atrial kick (e.g. atrial fibrillation)
- Intrathoracic pressure (reduces preload)
- Clinical surrogate
- Central venous pressure
Afterload
- Force opposing ventricular contraction during systole
- It is influenced by:
- Vascular resistance (e.g. hypertension, vasopressors)
- Outflow tract obstruction (e.g. aortic stenosis, HOCM)
- LV chamber size/volume (e.g. heart failure)
- Arterial compliance
- Positive pressure ventilation
- Clinical surrogate
- Systemic vascular resistance
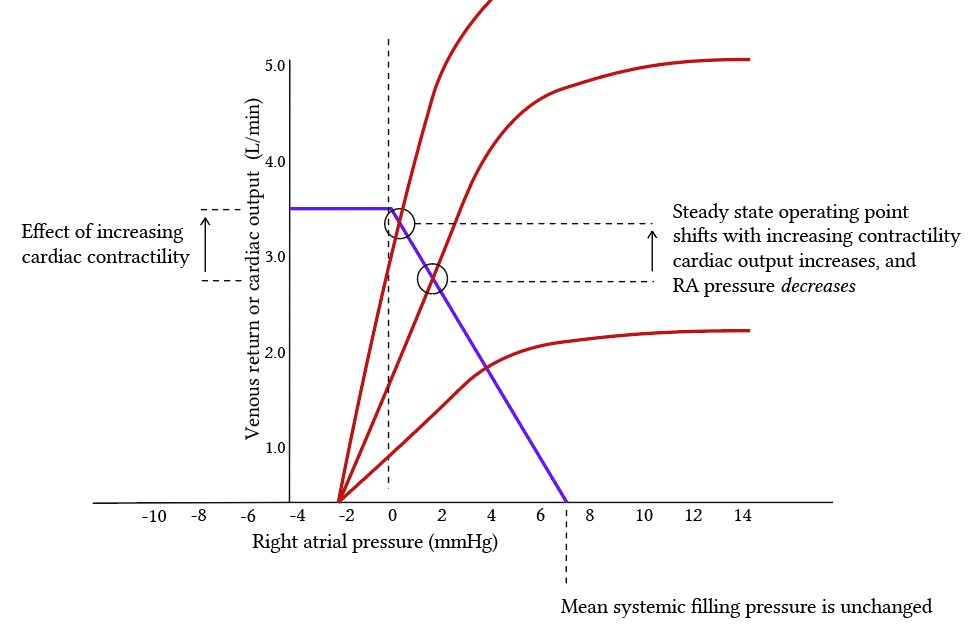
Contractility
- Intrinsic strength of myocardial contraction that is independent of preload and afterload and primarily influenced by the autonomic nervous system’s regulation of cystolic
- It is influenced by:
- Sympathetic and parasympathetic activation
- Ionotropes
- Beta blockers
- Calcium channel blockers
- Pathologic states which interfere calcium handling and ATP generation
- Ischaemia/infarction
- Inflammation (e.g. myocarditis)
- Acid-base derrangements
- Hypothermia
- Heart rate (bowditch effect)
- Clinical surrogate
- Ejection fraction
Stroke Volume and Ejection Fraction
- The volume of blood ejected from the left ventricle during systole
Cardiac Output and Cardiac Index
- Cardiac output is volume of blood ejected forward from heart per unit time (L/min)
- Cardiac index is the cardiac output adjusted for estimated body surface area (L/min/m^2)
- Normal is 2.5-4.0 L/min/m2
- Oxygen delivery () is the product of cardiac output and the oxygen content of arterial blood:
- If there is adequate arterial concentration, then cardiac output is the main determinant of
- Inadequate to meet (oxygen uptake) defines Shock
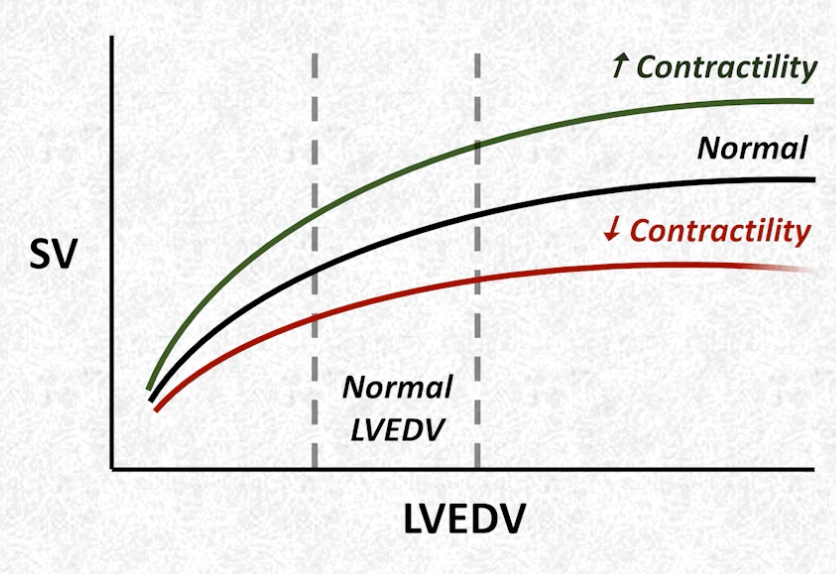
Frank-Starling Mechanism
- Stoke volume is dependent upon LV end-diastolic volume
Analogy
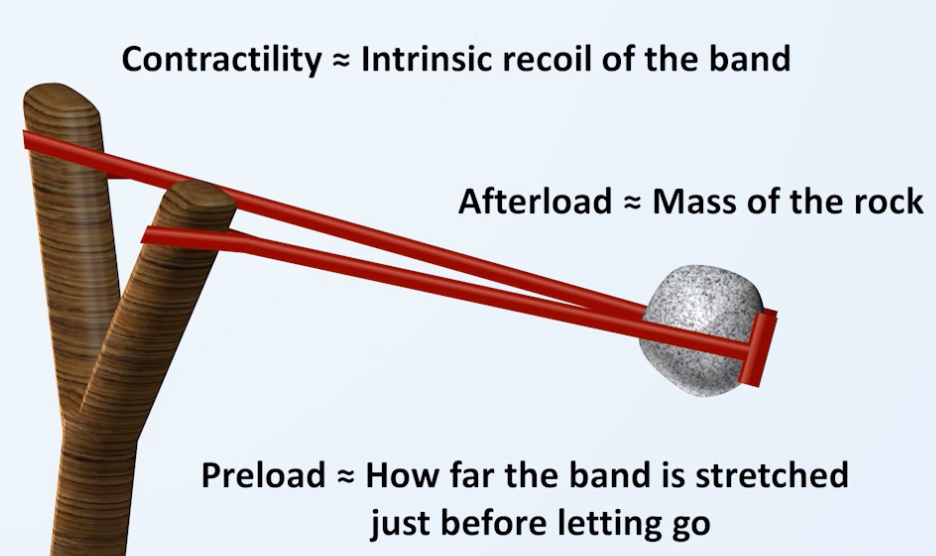
- Stoke volume here is how far the rock will travel when released
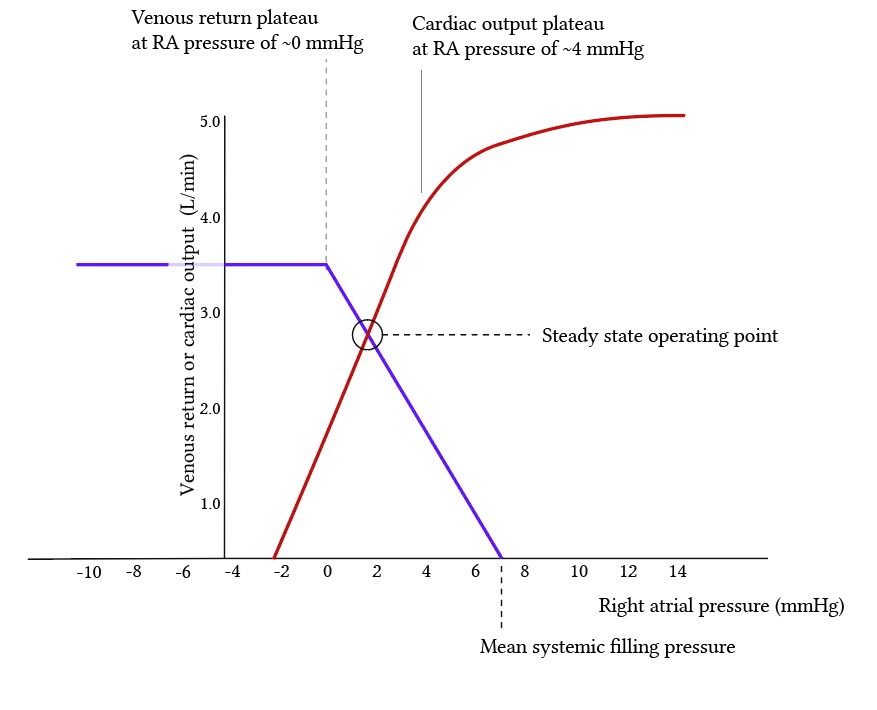
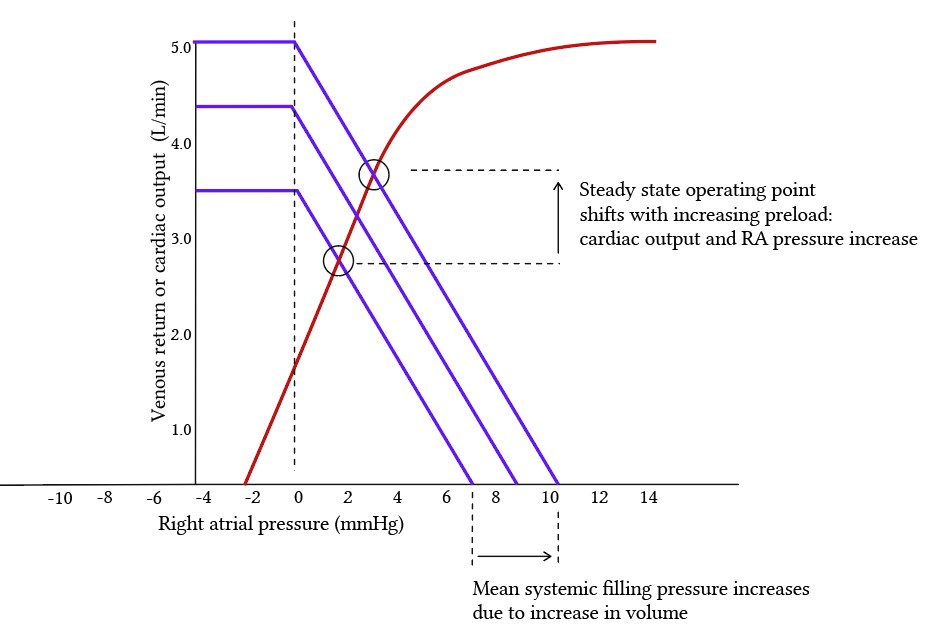
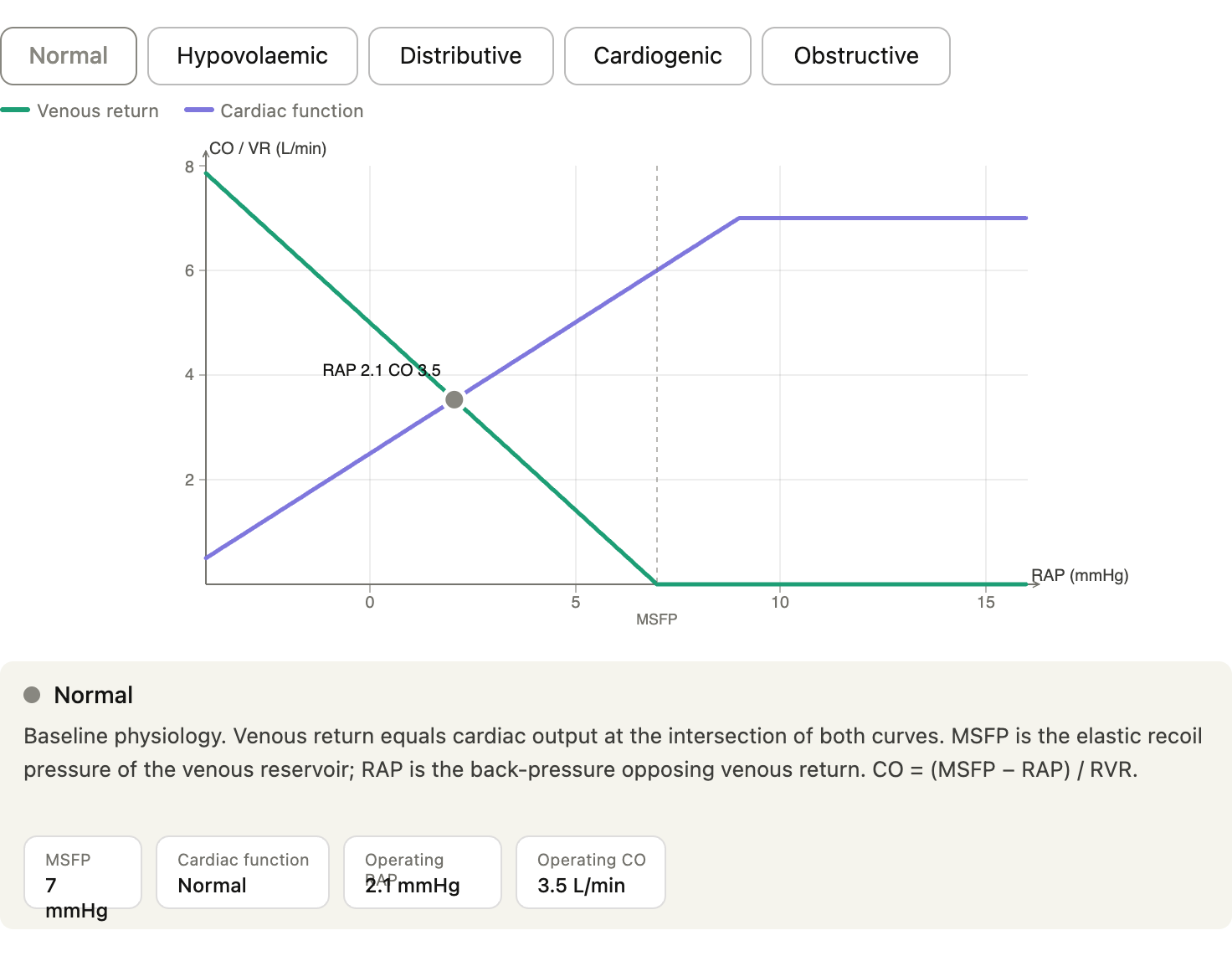
Venous Return
- At most circumstances
-
Where:
- MSFP is the mean systemic filling pressure, the pressure that would exist throughout the entire systemic vasculature if the heart stopped and flow equalised (i.e. elastic recoil pressure of the venous reservoir), normally 7-8 mmHg
- Increased by: volume loading, venoconstriction (adrenaline, noradrenaline)
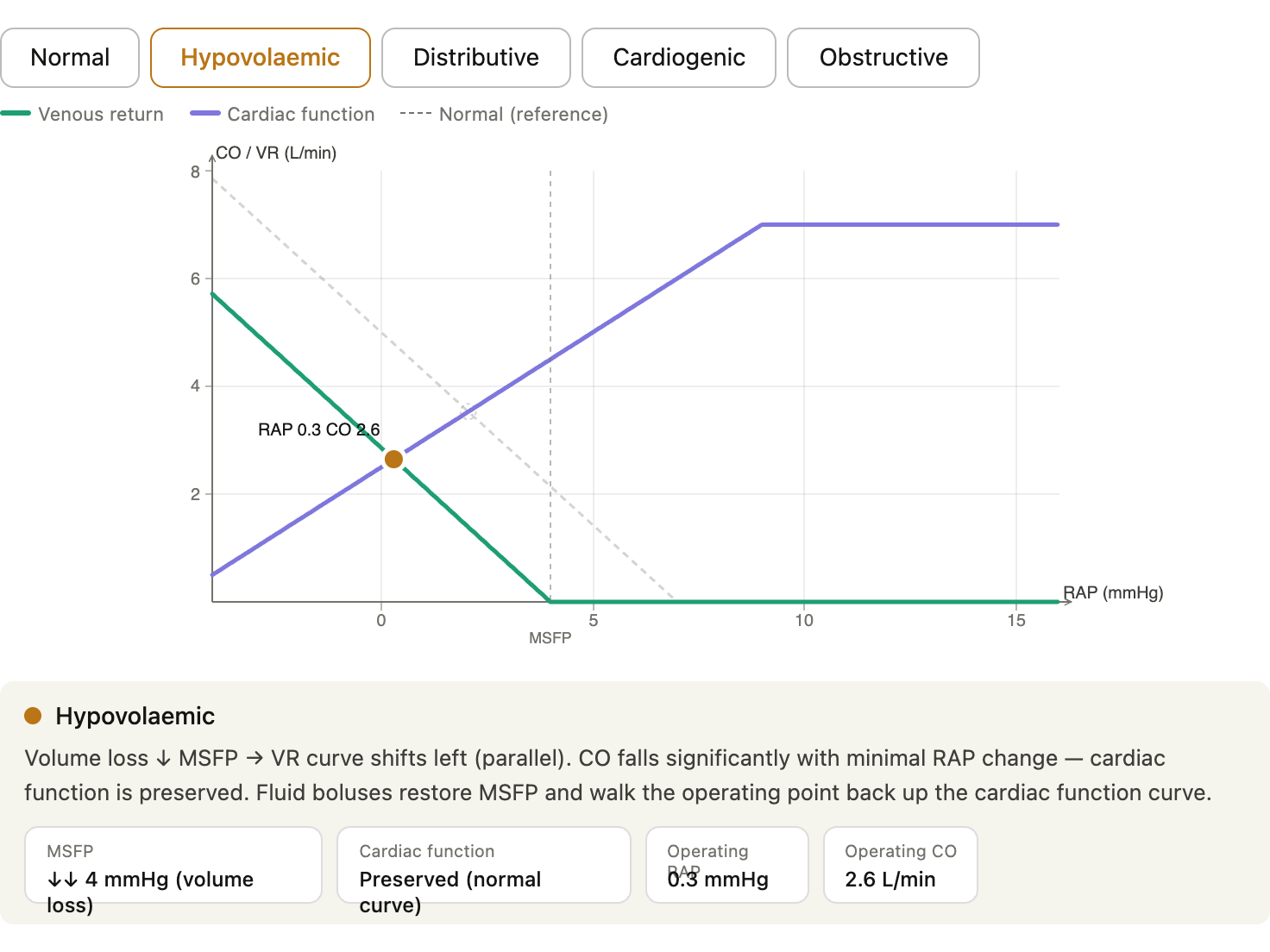
- Decreased by: haemorrhage, venodilation (early phase sepsis, nitrates)
- RAP is the right atrial pressure and is the pressure opposing venous return
- Increased by: RV failure, tamponade, PEEP
- RVR is resistance to venous return and is the resistance of venous capacitance vessels, mainly set by small veins and venules
- Increased by: venoconstriction
- Increased by: hepatic congestion, abdominal compartment syndrome, external compression
- MSFP is the mean systemic filling pressure, the pressure that would exist throughout the entire systemic vasculature if the heart stopped and flow equalised (i.e. elastic recoil pressure of the venous reservoir), normally 7-8 mmHg
-
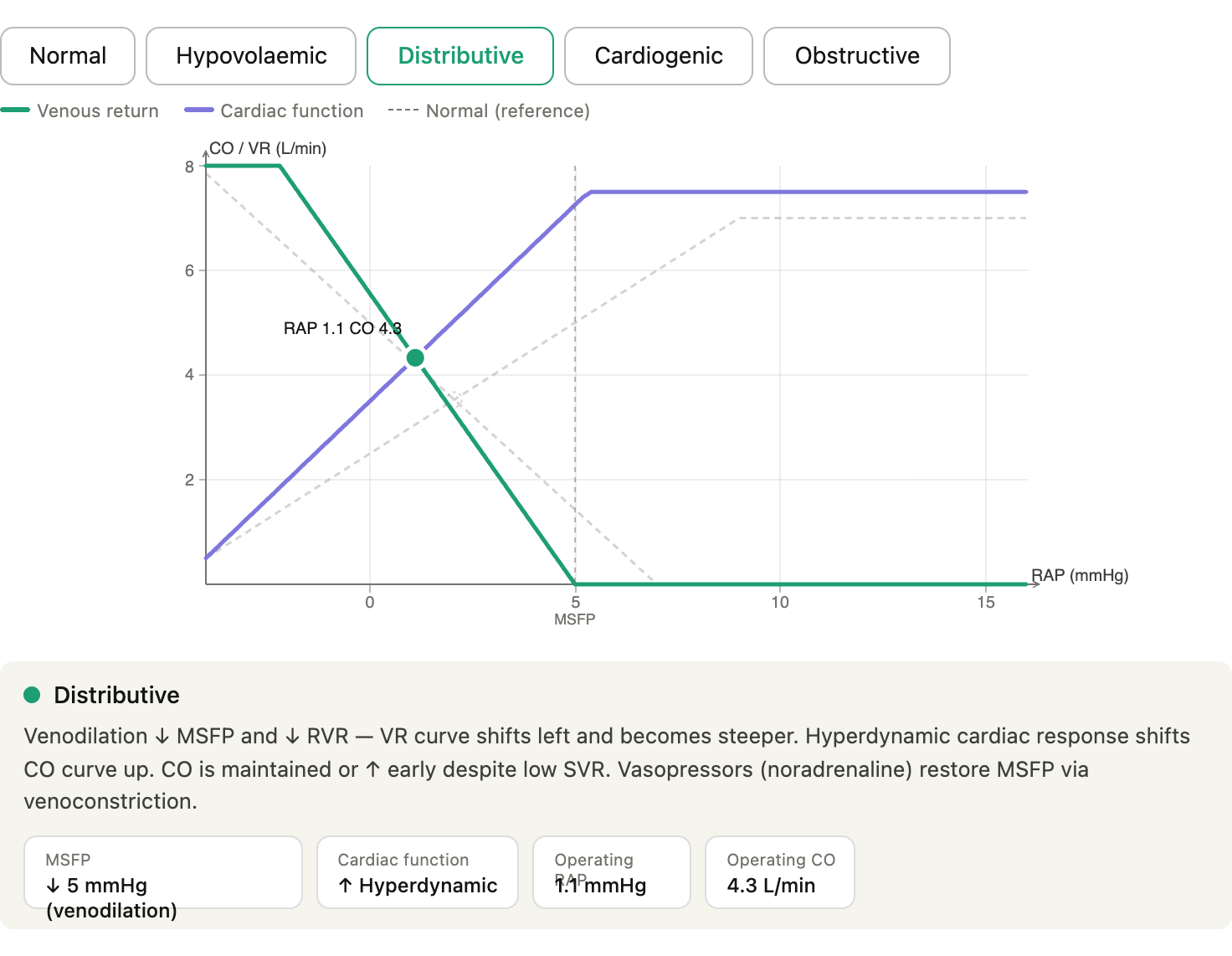
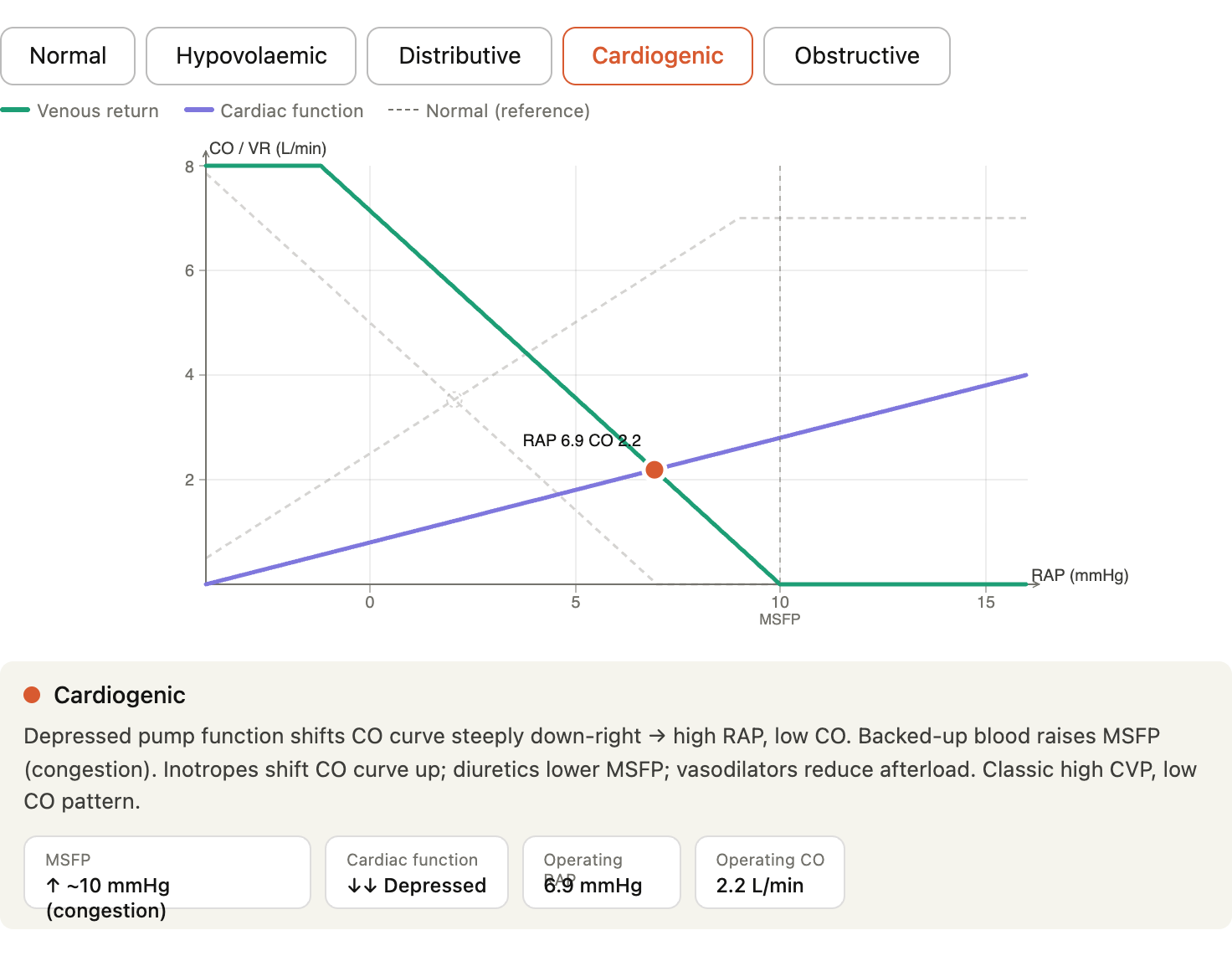
Fluid responsiveness: A patient is fluid-responsive if they’re on the steep part of both curves — giving volume will shift the VR curve right (raise MSFP) and walk up the cardiac function curve. If they’re on the flat part of the cardiac curve (RV failure, LV failure), fluid raises RAP without improving CO.
-
Vasopressors vs inotropes: Noradrenaline raises MSFP (venoconstriction) AND arterial resistance — in distributive shock, the venous effect is often why it helps CO as much as the arterial effect does. Inotropes shift the cardiac function curve upward.
-
Mechanical ventilation: PEEP → ↑ intrathoracic pressure → ↑ RAP → ↓ venous return → ↓ CO. You can partially compensate with volume (raise MSFP).
-
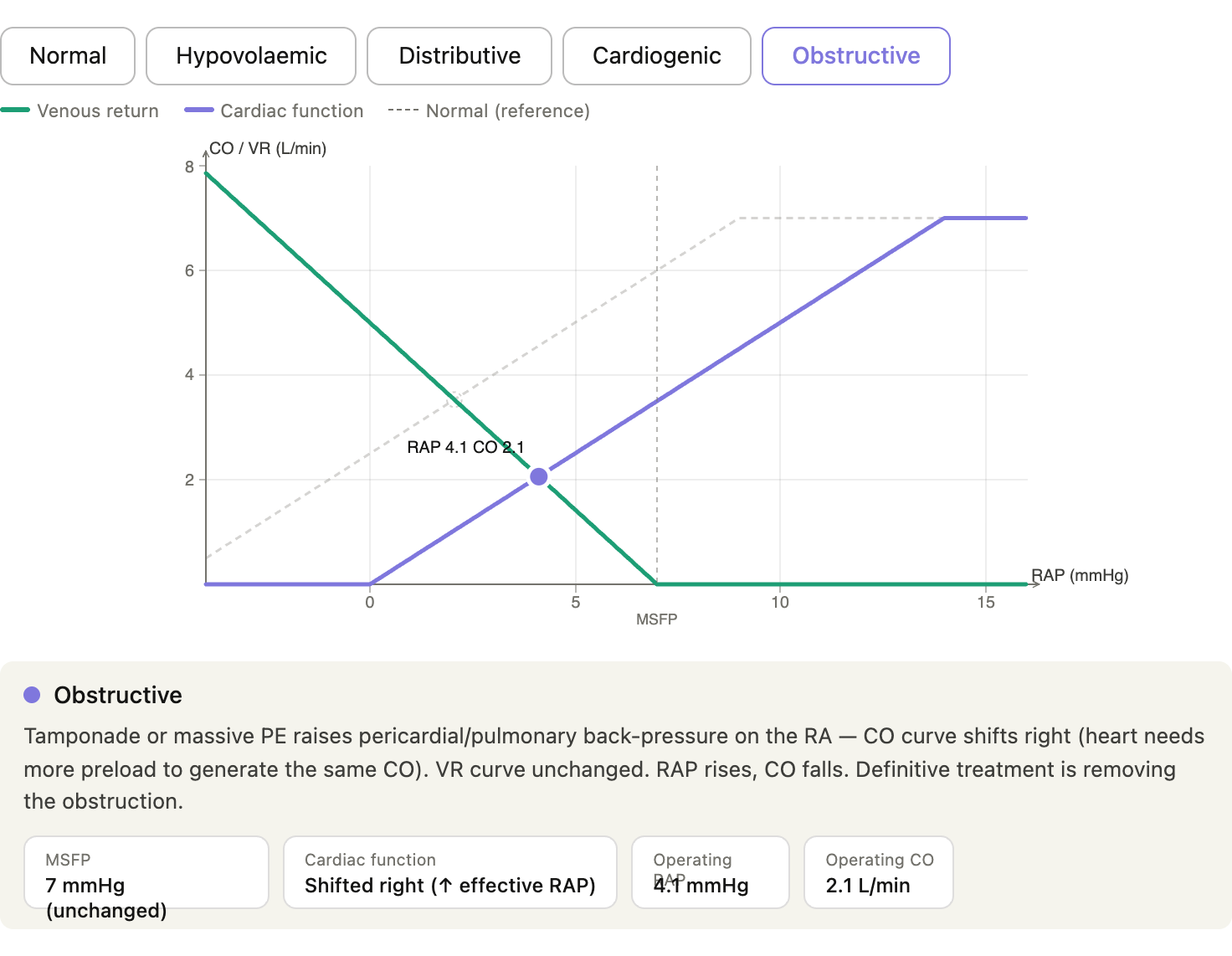
Tamponade physiology: The pericardial pressure compresses the RA, raising effective RAP → venous return drops despite normal MSFP. Drainage immediately lowers this backpressure — CO improves before you’ve given a drop of fluid.
-
Shock physiology: guyton-venous-return.html
Viscosity and Turbulence
- Turbulent flow is more likely when Renold’s number (Re) is high
- Renold’s number can be given by (where is the viscosity of fluid)