Dangerous arrhythmias are more common when hypokalaemia also occurs with QT prolonging drugs, digoxin toxicity, Hypomagnesaemia, coronary ischaemia
Assessment
History
fatigue
muscle cramps
weakness
constipation
rhabdomyolysis
ascending paralysis
respiratory failure
arrhythmias
symptoms more likely in pre-existing heart disease (IHD, CHF, LVH)
medications: cause of hypokalaemia and also anti-arrhythmics (sotalol → increased risk of arrhythmias)
Examination
Investigations
ECG
EUC
CMP
Digoxin level if on digoxin
Workup
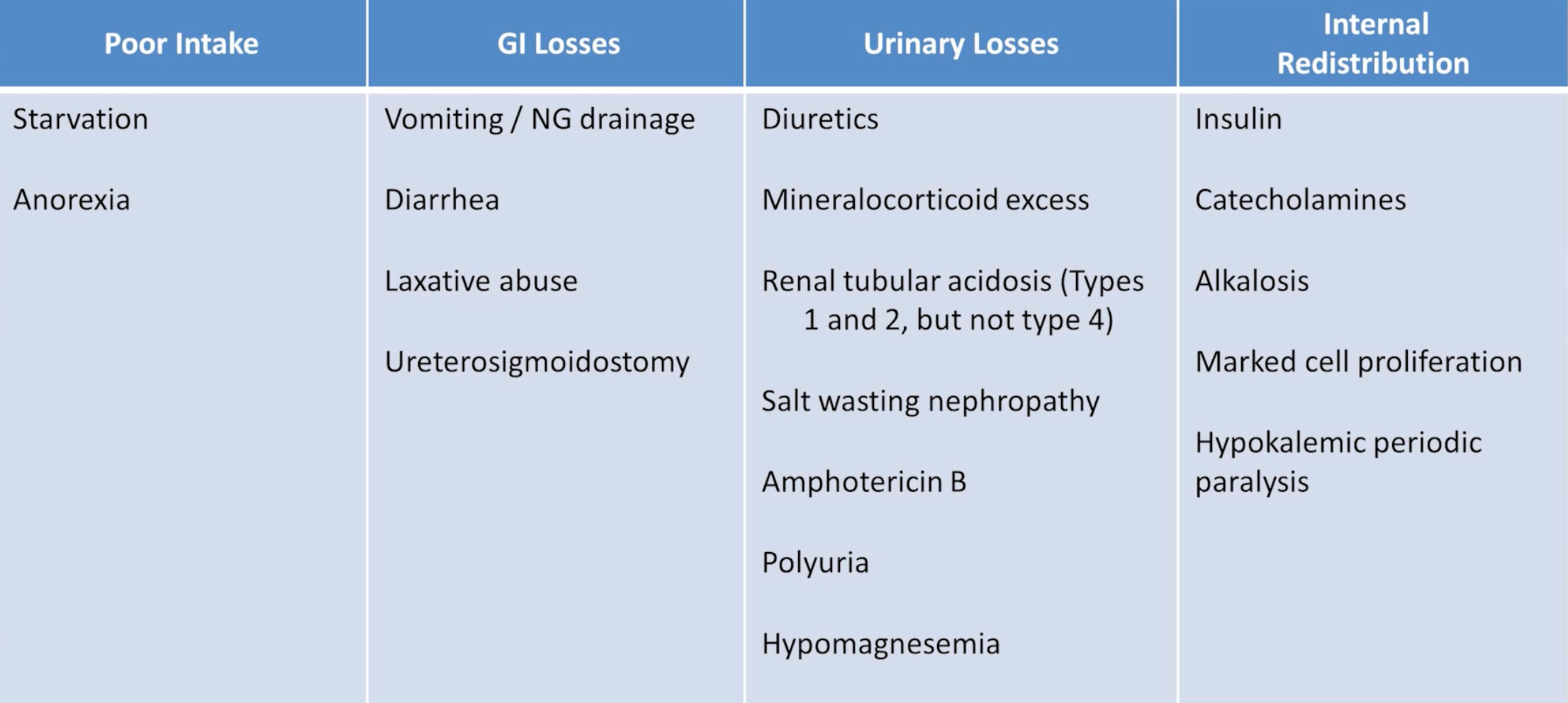
Most aetiologies are evident from history
Assess magnesium level
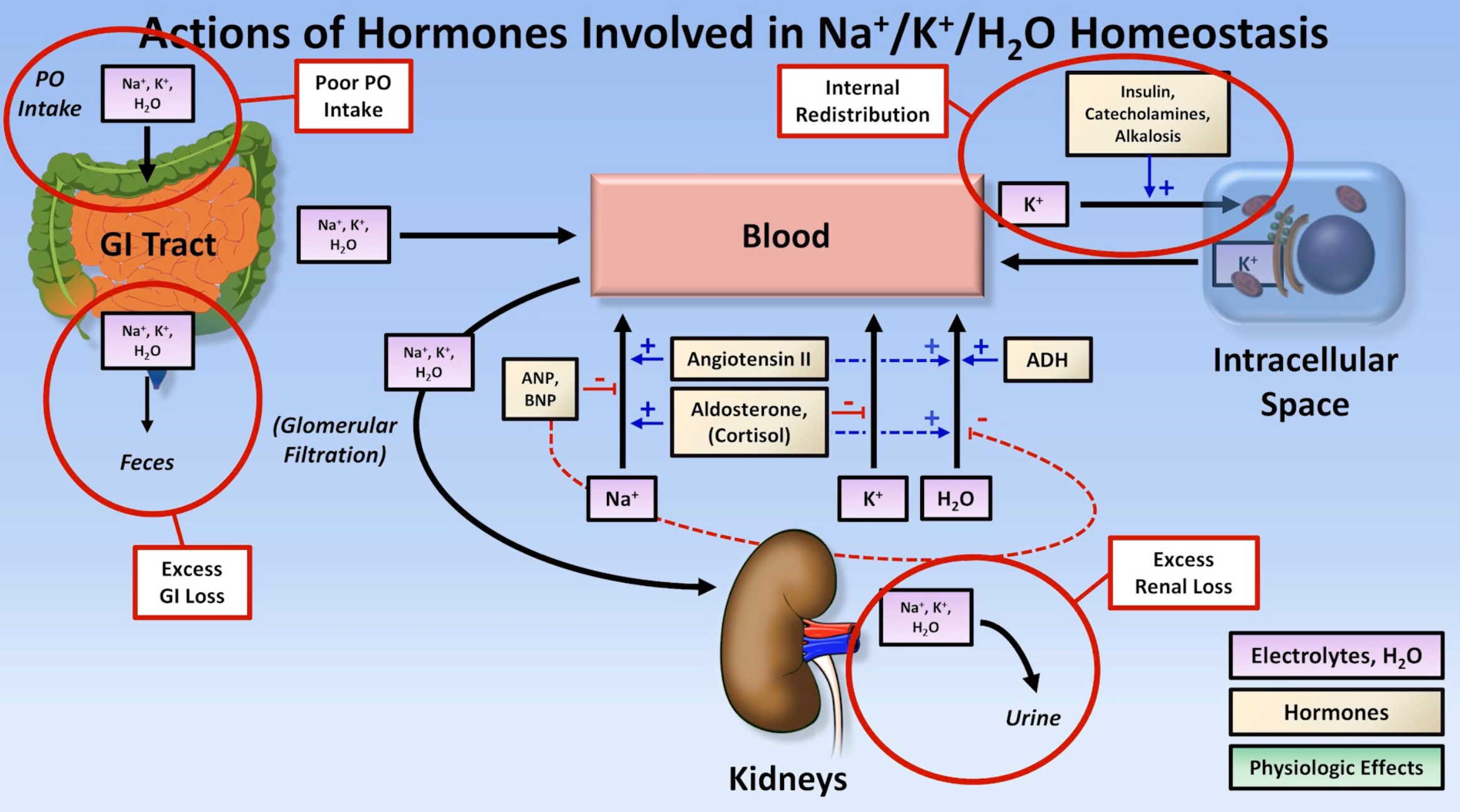
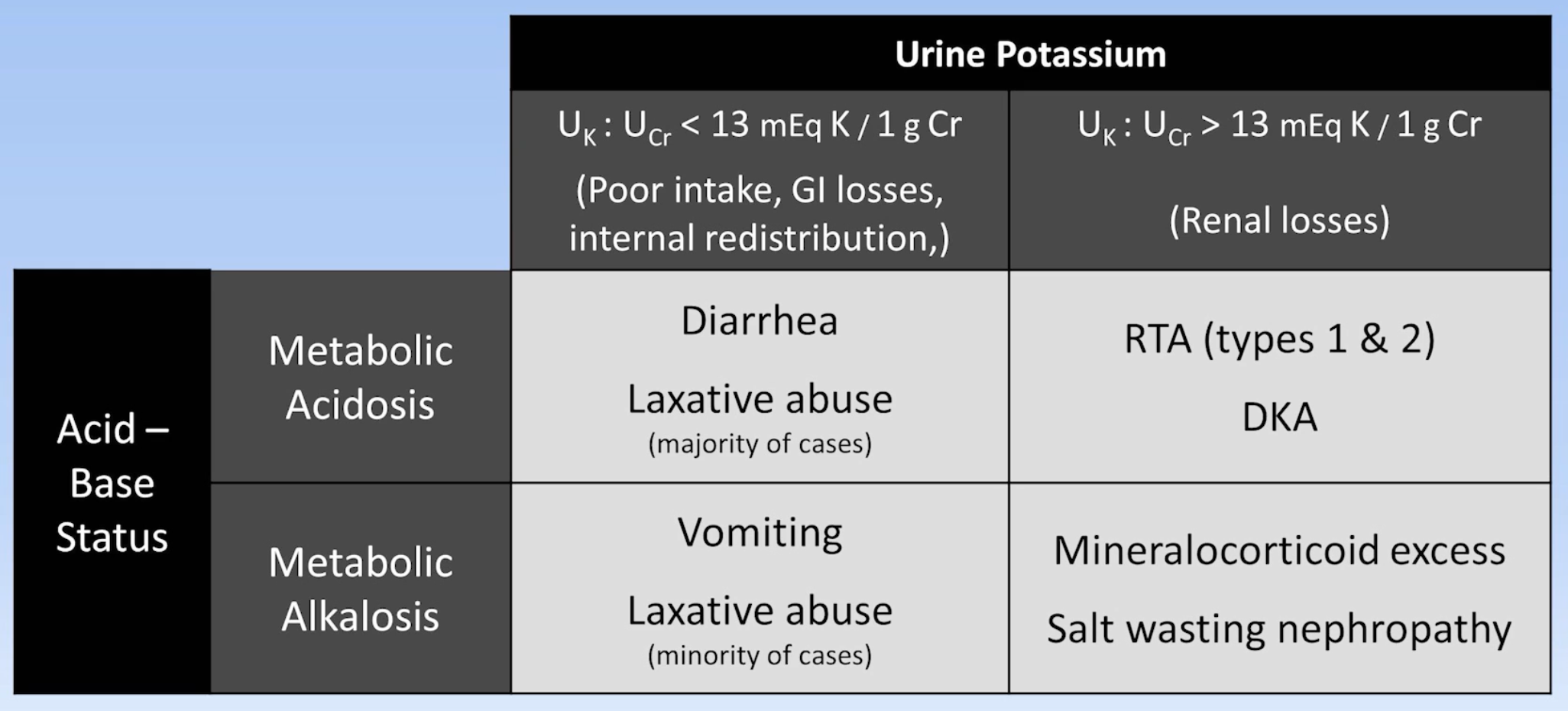
Check acid base status and measure urine potassium excretion
Management
Replace magnesium as fascilitates a more rapid correction of hyperkalaemia
For patients with hypokalaemia in the setting of essential diuretic use (e.g. heart failure) or hyperaldosteronism, a potassium-sparing diuretic is usually more effective than chronic potassium replacement