Aetiologies
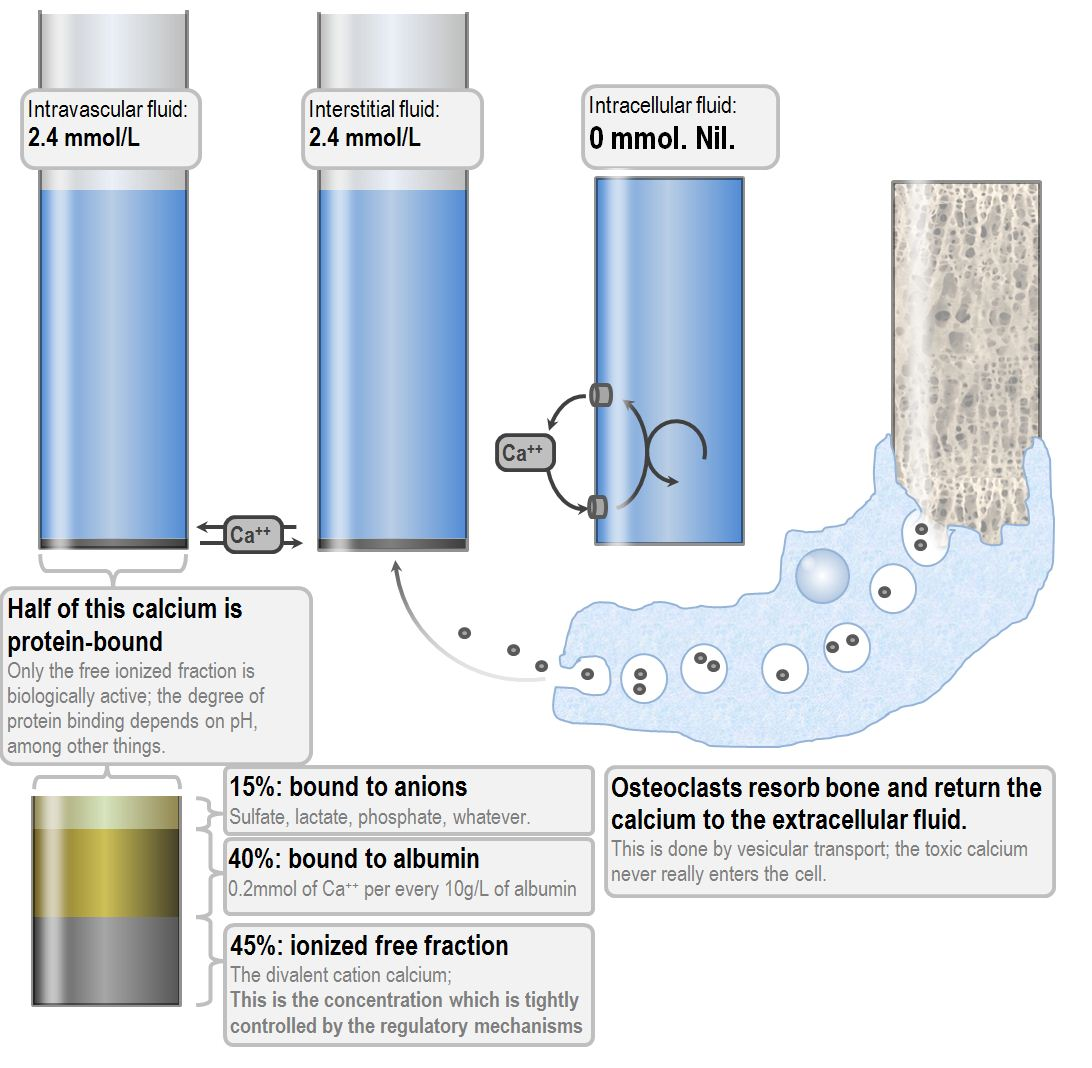
- Increased binding of calcium to protein
- Magnesium is required for the release of PTH ⇒ hypomagnesaemia can precipitate hypocalcaemia
| Factor | Effect on Ionised Calcium |
|---|---|
| Albumin | increased albumin = decreased ionised calcium |
| pH | increased pH = decreased ionised calcium |
| Lactate | increased lactate = decreased ionised calcium |
| Phosphate | increased phosphate = decreased ionised calcium |
| Bicarbonate | increased bicarbonate = decreased ionised calcium |
| Citrate | increased citrate = decreased ionised calcium |
| Heparin | Presence of heparin in the sample = decreased ionised calcium |
| Free fatty acids | Increase in free fatty acids = decreased ionised calcium |
- Low parathyroid hormone
- Primary Hypoparathyroidism (i.e. destruction of parathyroid glands)
- Dysregulation of PTH secretion (e.g. congenital, Hypomagnesaemia, Sepsis)
- High or normal parathyroid hormone
- Vitamin D deficiency (e.g. true deficiency as that in malabsorption, insufficient synthesis as in renal failure)
- Altered protein binding (e.g. alkalosis)
- PTH resistance (e.g. Hypomagnesaemia)
- Chelation or depletion
- Hyperphosphotaemia
- Tumour lysis syndrome
- Acute pancreatitis
- Consumption by osteoclastic bone metastases
- Drugs
- Citrate
- Phosphate
- Biphosphonates
- Phenytoin
- Causes of hypocalcaemia categorised by acid base balance:
- Metabolic alkalosis – citrate toxicity
- Metabolic acidosis – acute renal failure, tumour lysis, rhabdomyolysis, pancreatitis, ethylene glycol poisoning, hydrofluoric acid, sepsis, burns
- Citrate toxicity is probably the only cause of low ionised calcium with normal total calcium
- This is because measurement instruments which detect calcium will also measure citrate-calcium complexes in the serum, but the electrode which measures ionised calcium will only measure the free fraction, which decreases with citrate chelation
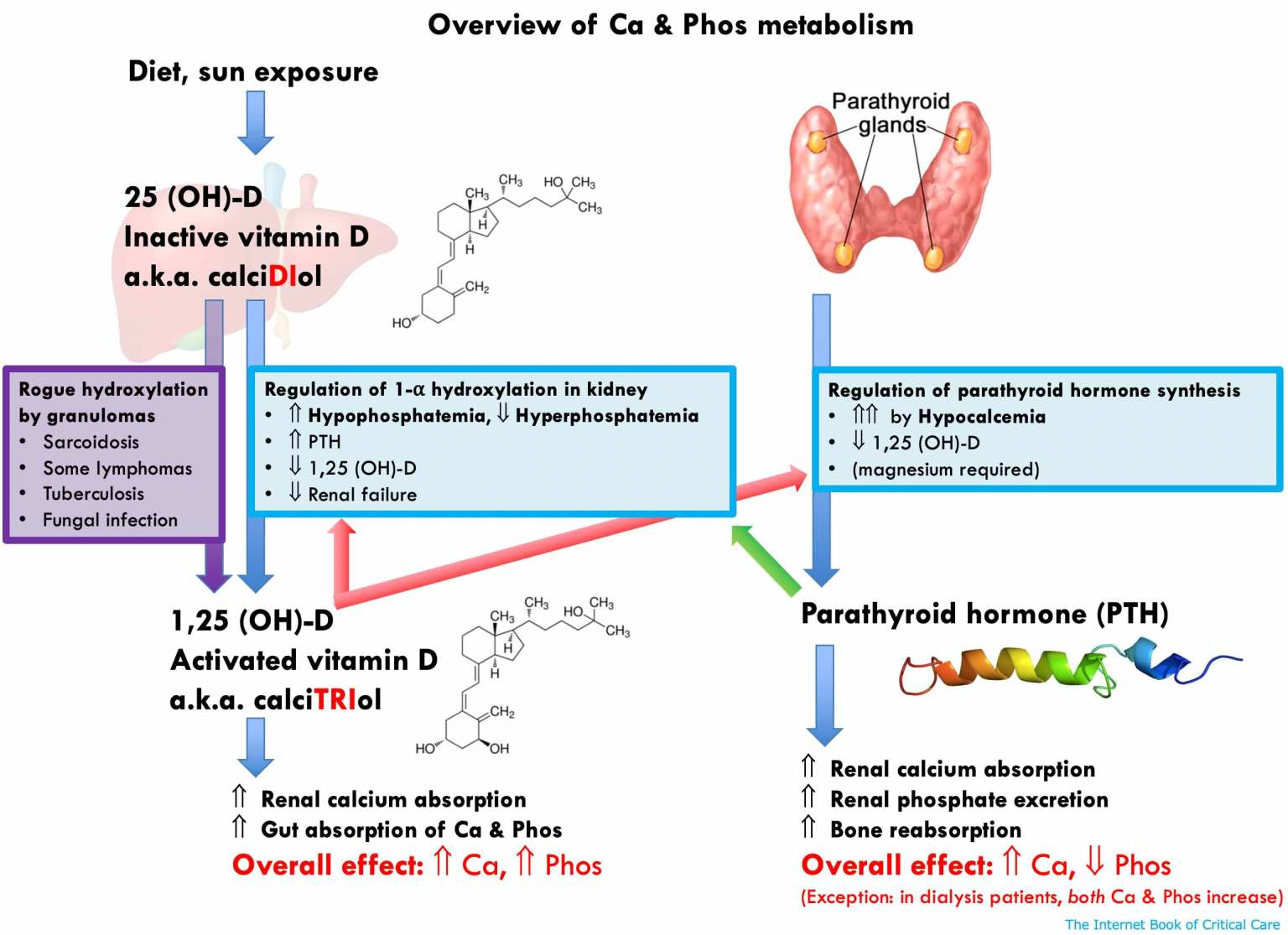
Physiology of Calcium Homeostasis
Parathyroid Hormone
- Secreted by chief cells of the parathyroid glands
- Most regulatory influences on PTH are inhibitory influences (inorganic phosphate is the only proper stimulatory release factor)
- Calcium level and PTH secretion relation is not linear; high calcium can never completely suppress PTH secretion and PTH secretion reaches a peak at calcium concentration of around 0.90 mmol/L
- Effects of PTH
- Osteoclastic:
- Direct effect on decreasing osteoblast activity
- Increased osteoclast activity
- Thus, increased release of calcium and phosphate from bone, and decreased bone deposition
- Renal:
- Decreased reabsorption of inorganic phosphate at the proximal tubule
- Increased reabsorption of calcium at the thick ascending limb of the loop of Henle
- Increased production of production of calcitriol in the kidney, through the stimulation of renal 1α-hydroxylase.
Calcitonin
- Secreted from parafollicular cells of the thyroid gland
- Osteoclastic:
- Direct effect on decreasing osteoclast activity1
- This decreases the resorption of bone, and therefore limits the entry of bone calcium and phosphate into the blood
- Renal:
- Calcitonin acts as a weak diuretic, increasing the elimination of sodium, chloride, phosphate and calcium. The effect on calcium is mainly due to inhibited reabsorption.
- It also increases production of production of calcitriol in the kidney, through the stimulation of renal 1α-hydroxylase.
- Intestinal:
- Calcitonin increases gastric acid and pepsin secretion and decreases pancreatic amylase secretion.
- It has no direct effect on calcium absorption in the intestine, but it can increase it indirectly by stimulating renal calcitriol synthesis
Action of Biphosphonates
Link to original
- Inhibition of osteoclast and osteoblast activity
- Osteoclasts:
- Inhibition of osteoclast recruitment and adhesion
- Shortening of the life span of osteoclasts
- Inhibition of osteoclast activity by inhibiting several essential parts of the cholesterol synthesis pathway
- Inhibition of calcification by inhibiting the formation of calcium phosphate salts
- Mainly seen in high doses
- A totally physicochemical effect: they bind to the calcium of calcium phosphate
- The result is inhibition of formation and aggregation of calcium phosphate crystals and inhibition of the transformation of amorphous calcium phosphate into hydroxyapatite.
Clinical Features
- Mild hypocalcaemia
- Generalised myalgia
- Twitching, fasciculations
- QT prolongation
- Chvostek sign is the twicth elicited by tapping over the facial nerve.
- Confusion, delirium psychosis
- Severe hypocalcaemia
- Trousseau is the carpopedal spasm in response to overlong BP cuff inflation.
- Tetany and seizures
- Papilloedema and raised intracranial pressure
- Cardiac arrhythmias (e.g. Torsades)
- Hypotension
Investigations
- ECG
- PTH
- PTH normally rises in resposne to hypocalcaemia
- Low PTH suggests dysregulation of PTH secretion which can be due to primary Hypoparathyroidism (e.g. surgical destruction), PTH secretion suppression as in sepsis or congenital mutations
- Serum 25-hydroxyvitamin D
- Low vitamin D can cause hypocalcaemia
- Low vitamin D can be secondary to lack of UV light, dietary deficiency or renal failure (hence urea and creatinine)
- Urea and creatinine
- Magnesium and phosphate level
- Hypomagnesaemia causes both decreased PTH secretion and impaired tissue response to PTH but requires Mg levels < 0.4 mmol/L
- Hyperphosphataemia can be associated with low calcium
- Primary Hypoparathyroidism disorders are associated with a raised serum phosphate
- Secondary Hyperparathyroidism (e.g. in Vitamin D deficiency) are associated with a low phosphate
- High phosphate will also chelate calcium; forming insoluble calcium phosphate
- Amylase and lipase
- Albumin
- CK and urate level to observe for rhabdomyolysis
- Correcting for albumin, however evidence demonstrates that formulas actually perform worse than uncorrected calcium levels
Management
- Acute replacement
- IV replacement with calcium salt (chloride has more calcium per 10mL)
- 10mL gluconate = 2.3mmol = 93mg, 10mL chloride = 6.8mmol = 272mg
- Calcium chloride has more significant phlebitis risk and tissue necrosis if extravasation; only give via a central line
- Calcium gluconate is preferred in peripheral access
- Calcium chloride is preferred in cardiac arrest, severe hepatic impairment or when central access already exists
- Ensure magnesium and phosphate replacement also occurs accordingly
- IV replacement with calcium salt (chloride has more calcium per 10mL)
- Medium term placement
- Oral replacement with either calcium citrate or carbonate1
- Vitamin D replacement
- With intact parathyroid function (i.e. PTH appropriately high) cholecalciferol (converted to calcitriol in the kidney when parathyroid function is normal)
- With impaired parathyroid function give calcitriol
- Recalcitrant hypocalcaemia
- Thiazide diuretics
- Recombinant PTH
Sources
Footnotes
-
Perhaps calcium citrate is better as it does not need to be taken after food as it does not require a normal gastric pH to dissolve; calcium citrate might therefore be appropriate for fasted patients ↩