Also see: Shock for the management of undifferentiated shock
- SOFA Score can be used for sepsis severity score
- ≥2 ⇒ ↑ mortality
- Antibiotics
- Tazoscin
- Vancomycin
- ±Azithromycin if suspicious of respiratory cause
Diagnostic Criteria
Sepsis-3 Criteria
life-threatening organ dysfunction due to a dysregulated host response to infection Organ dysfunction is suggested by:
- An increase of ≥2 points of the SOFA score (SOFA-2) Septic shock is definted as above as well as both:
- Hypotension requiring vasopressors
- Lactate >2 mmol/L
Screening
- Who to screen
- All acutely ill patients who arrive to hospital by ambulance or flight
- Consider screening with SIRS criteria or MEWS as opposed to qSOFA
Investigations
- Bedside
- ECG - ischaemia, arrhythmias UA and urine culture
- Bloods
- Blood cultures x2
- FBC - anaemia, thrombocytopaenia
- DIC panel (e.g. INR, aPTT, fibrinogen)
- EUC - AKI
- ABG - quantify P/F ratio, hypercapnoea, pH status and lactate
- LFTs - ischaemic hepatitis, hyperbilirubinaemia
- Troponin
- Imaging
- Chest X-ray - assess respiratory source and pulmonary oedema
- Echocardiogram - sepsis-induced cardiomyopathy
- Abdominal imaging
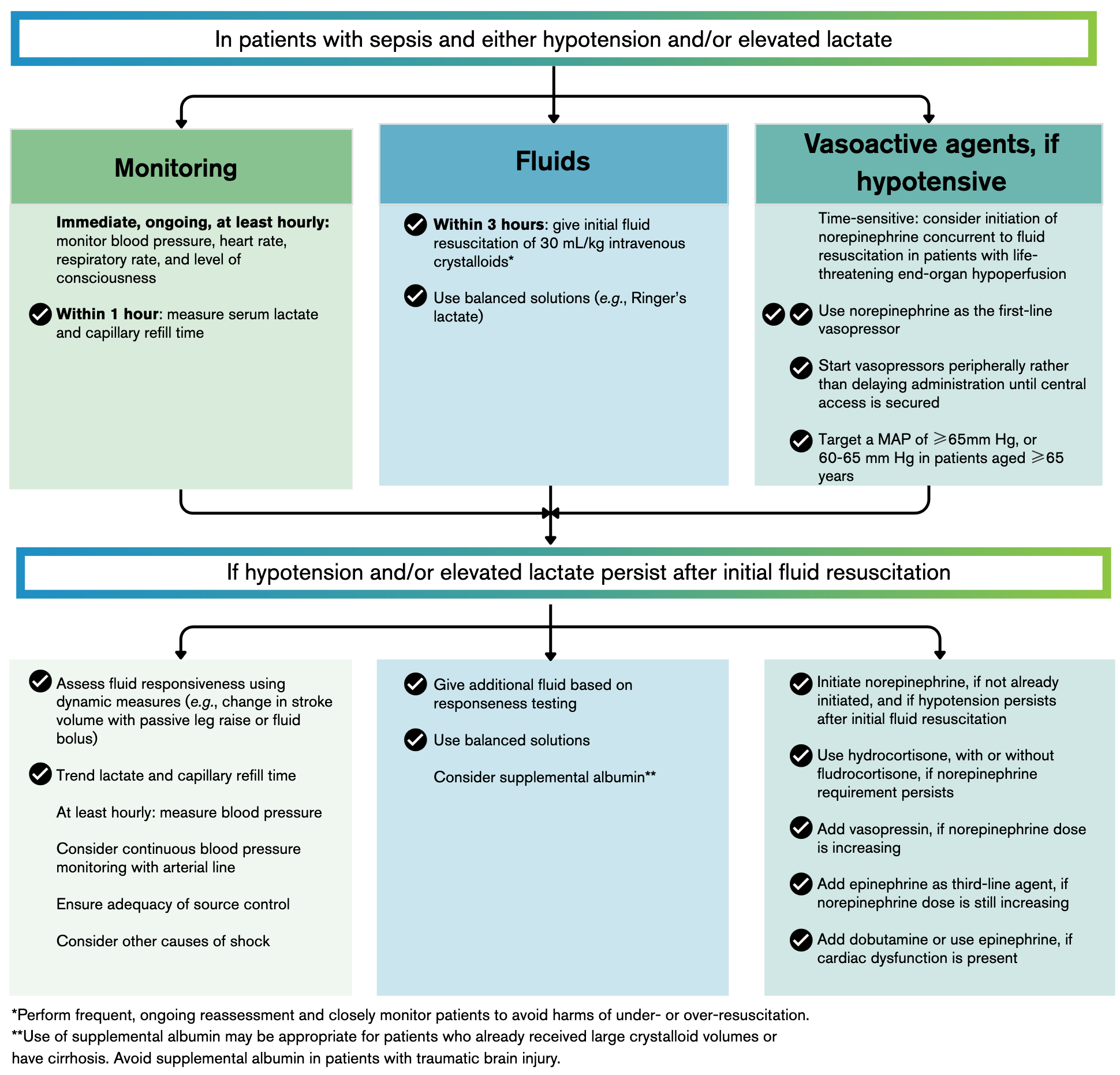
Management
Summary of Management
- IV access and blood cultures
- Early (within 1 hour) antibiotics
- Fluid resuscitation: 30mL/kg
- Albumin
- Assess fluid resuscitation with haemodynamic monitoring and lactate
- Vasopressors (noradrenaline as first line)
- Consider ionotropes for septic cardiomyopathy
- Refractory shock: consider vasopressin and corticosteroids
- If still refractory consider: intravenous calcium, methylene blue, esmolol
- Consider toxic shock: IV immunoglobulin and clindamycin
Fluid Resuscitation
- Large-bore cannulae
- Blood cultures; ideally two sets from different sites
- Antibiotic therapy without delay
- Ideally within 1 hour of recognition if patient is in shock
- If not in shock, where sepsis is probable but not confirmed; rapid assessment and administer antimicrobial therapy within 3 hours
- Consider anaerobic coverage when risk factors exist e.g. intra-abdominal or deep seated gynaecological/obstetric source of infection, necrotising soft tissue infection, head and neck infection and central nervous system abscesses or empyema
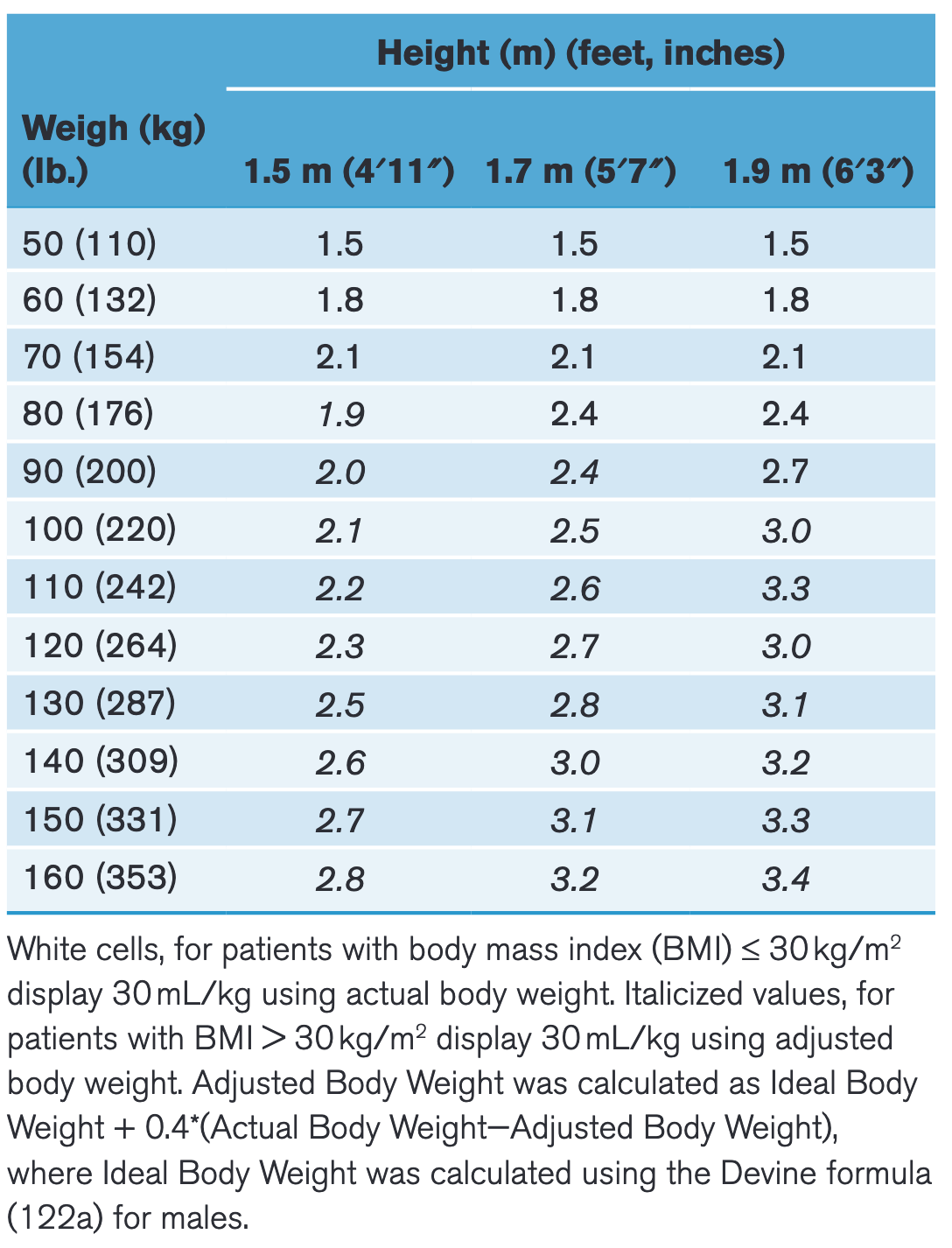
- 30mL/kg of crystalloid fluid (preferably balanced fluids e.g. hartmanns, plasmalyte)1 within the first 3 hours
- Weight-based fluid volume should be calculated on actual body weight (particularly in underweight patients) or adjusted body weight in patients with BMI > 30 (see: adjusted body weight calculator or table below)
- In patients with traumatic brain injury use 0.9% saline
- Albumin
- Transfuse blood if Hb < 70 but remain conservative in transfusion efforts
Assess Need for Further Fluid Resuscitation
- Monitoring
- Arterial line
- Central line if pressors are required
- Monitor capillary refill time where serial lactate measurements are not possible
- Goals
- Aim for MAP of 65±5 mmHg and lower MAP range of 60-65 mmHg in patients aged ≥ 65 years
- Aun for CVP 8-12 mmHg
- Measure fluid responsiveness (e.g. pulse pressure variation, expiratory hold manoeuvre, passive leg raise, stroke volume variation, IVC ultrasonography)
- Fluid resuscitation is considered adequate if:
- > 70%
- Lactate clearance is better than 10% over 2 hours
- Arteriovenous difference < 6 mmHg
- Urine output > 1.0 mL/kg
- There does not appear to be a mortality benefit with using a restricted fluid approach and early vasopressors than the standard approach involving grater fluid volume and later administration of vasopressors (Vasopressors or Fluids in Early Septic Shock, The ARISE FLUIDS Investigators, June 2026 DOI: 10.1056/NEJMoa2516225)
Vasopressors
- If no further fluid resuscitation can be provided and haemodynamics still suboptimal start pressors
- Noradrenaline remains first choice
- Start vasopressors peripherally (e.g. with metaraminol) to avoid delaying initiation of vasopressors until central venous access is secured
Assess Adequacy of Cardiac Output
- Features of septic cardiomyopathy
- Rapid onset
- Reversible and leads to full recovery in survivors, usually over 7-10 days
- Left ventricular dilatation with normal or low filling pressure (due to increased LV compliance and EDV and coexistent RV dysfunction)
- Global ventricular dysfunction with decreased ejection fraction (due to ventricular dilatation despite preserved stroke volume)
- Absence of regional dysfunction (distinct from Takotsubo cardiomyopathy and myocardial ischaemia)
- Consider inotropes in patients:
- Low cardiac output that is being monitored
- Patients whose fluid resuscitation remains inadequate (as above: , lactate clearance etc.) despite adequate MAP
- Dobutamine appears to be most recommended followed by adrenaline?
Refractory Hypotension
- Refractory shock is suggested by:
- Patient has adequate preload
- Patient has adequate cardiac output
- MAP won’t remain in goal despite large doses of noradrenaline (>15 µg/min or 0.21 µg/kg/min or is otherwise causing arrhythmias)
- Fluid resuscitation measures remain inadequate
- Consider:
- Vasopressin (if available)
- If still inadequate consider adrenaline
- Steroids
- Toxic shock
- Vasopressin (if available)
- Other considerations:
- Correct ionised calcium
- Methylene blue
- Angiotensin-II
- Correct acidosis with bicarbonate if pH < 7.15
- Slow heart rate with esmolol2
- High volume haemofiltration
Source Control and Antibiotics
Other Therapies
- Potentially vitamin C, thiamine and hydrocortisone
Source:
- 16+ years old: https://www.cec.health.nsw.gov.au/__data/assets/pdf_file/0005/291803/Adult-Sepsis-Pathway.PDF
- Title Unavailable | Site Unreachable
- Derranged Physiology: Sepsis and Infections Chapters:
- Surviving Sepsis Campaign | SCCM
- 2026 SSC Adult Guidelines Updates: What Clinicians Need to Know - YouTube
- Critical Care Medicine | Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock 2026
- Septic cardiomyopathy • LITFL • CCC
- https://www.nejm.org.acs.hcn.com.au/doi/full/10.1056/NEJMoa2516225