Aetiologies
- Acute drop in LV function
- Volume dysfunction
- Volume overload (e.g. diuretic non-adherence, dietary indiscretion, iatrogenic volume resuscitation)
- Acute hypovolaemia
- Renal failure
- Arrhythmia
- Valvular dysfunction (e.g. LV outflow tract obstruction, prosthetic valve dysfunction, native valve dysfunction)
- Medications
- Non-adherence with heart failure therapies
- Adverse medication effect
- Sympathomimetic abuse
- Other
- Uncontrolled hypertension
- Uncontrolled sleep-disordered breathing
- Hypophosphatemia
- Iron deficiency (with or without anemia)
- Thyroid disease (hypothyroidism or hyperthyroidism)
- Infection/Sepsis
Diagnosis
SCAI Shock Classification
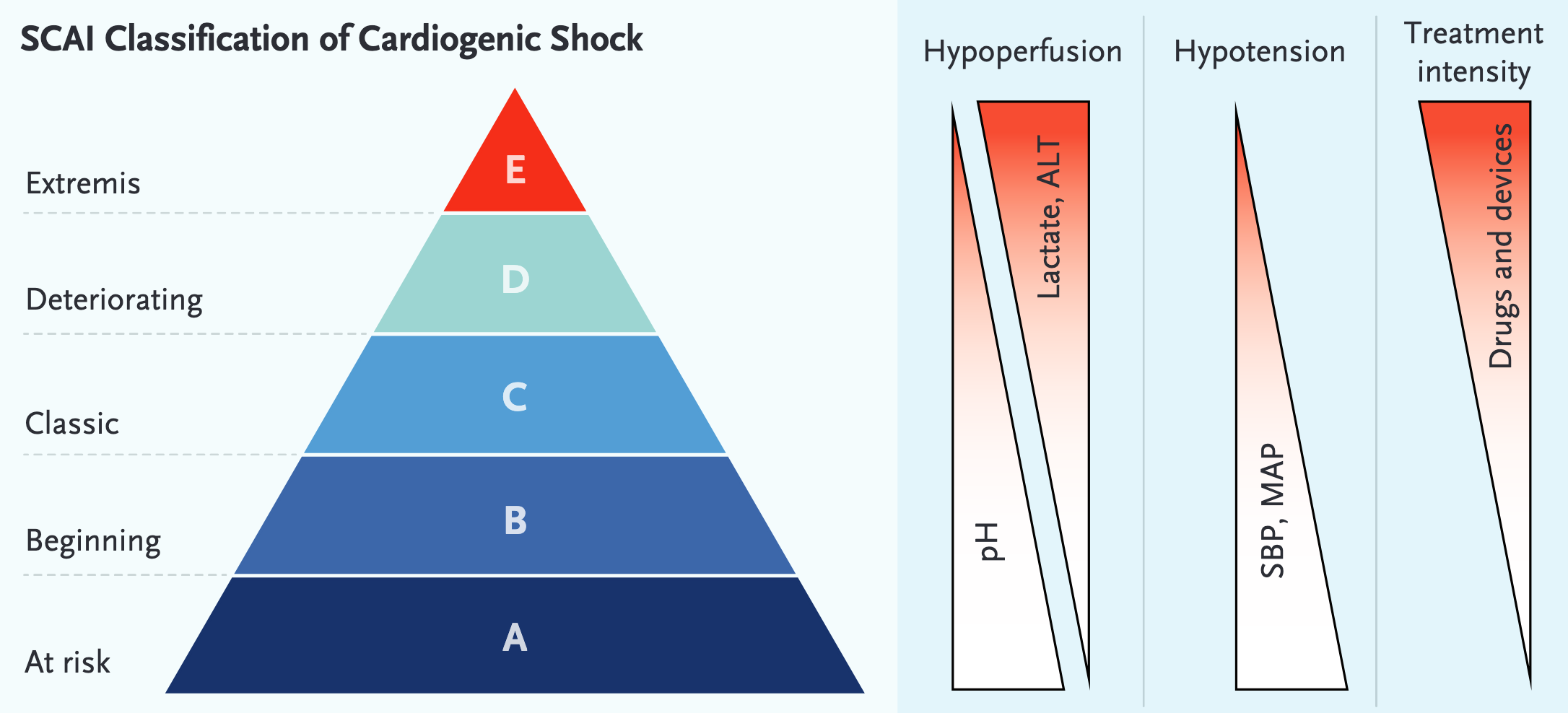
- A: At risk (mortality 0.8 - 28.9%)
- Not currently in shock but at risk with normal examination, biochemical markers and haemodynamics
- B: Beginning cardiogenic shock (mortality 2.2 - 35.1%)
- Defined as clinical instability without hypoperfusion
- Physical examination: warm and well perfused, elevated JVP and may have crackles
- Biochemical markers: normal lactate, minimal Acute Renal Failure, elevated BNP
- Haemodynamics:
- Hypotension (SBP <90 mm, MAP <60 mm, or >30 mm drop from baseline).
- Tachycardia (HR >100 b/m).
- Patients may have abnormal invasive hemodynamics (such as reduced cardiac output) but without end-organ malperfusion
- C: Classic cardiogenic shock (mortality 10.7 - 59.1%)
- Hypoperfusion & requires at least one intervention beyond volume resuscitation with patients usually relatively hypotensive but this isn’t a requirement
- If a patient requires vasoactive therapy, they are automatically classified as at least SCAI-C
- Physical examination:
- Volume overload
- May have altered mental status
- May appear cool/clammy and poorly perfused (delayed capillary refill, urine output <30 ml/hr)
- Biochemical markers:
- Lactate ≧2 mm
- AKI
- Increased LFTs
- Elevated BNP
- Haemodynamics
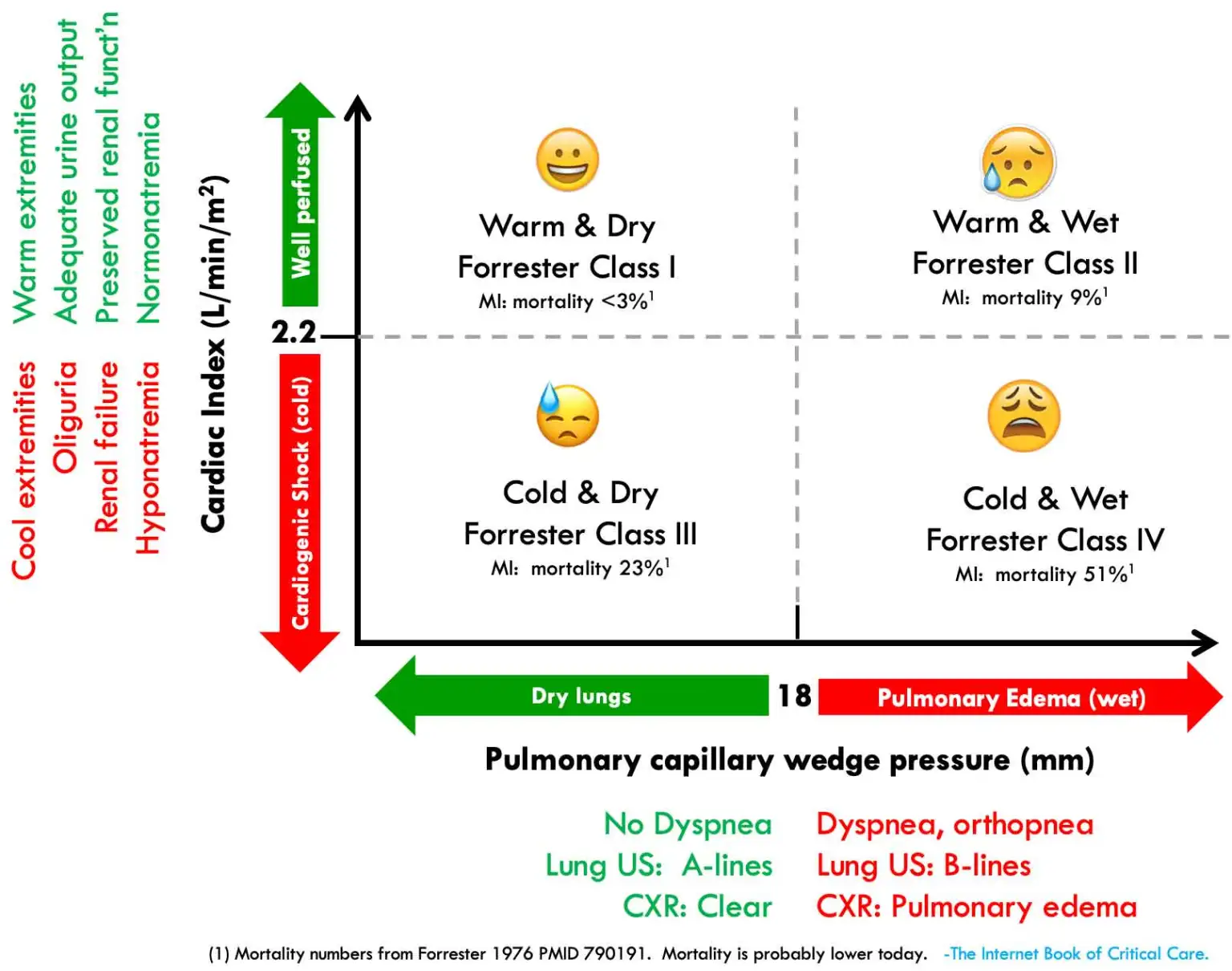
- Cardiac index
- PCWP > 15 mm
- Hypoperfusion & requires at least one intervention beyond volume resuscitation with patients usually relatively hypotensive but this isn’t a requirement
- D: Deterioration over time (mortality 24 - 66.9%)
- Worsening SCAI-C where the initial support strategy is failing
- The need for ≥2 vasoactives/devices due to failure of one intervention indicates SCAI-D
- The need for higher mechanical support or medication doses over time suggests SCAI-D
- Physical examination is same as SCAI-C plus not responding to therapy
- Biochemical markers are the same as SCAI-C plus worsening (e.g. lactate rising and persistently > 2 mmol/L)
- Haemodynamics are the same as SCAI-C plus requiring more support
- Worsening SCAI-C where the initial support strategy is failing
- E: Extremis (mortality 37.7 - 85.9%)
- Actual or impending circulatory collapse
- Near dead
- Lactate ≥8 mmol/L
- Profound hypotension despite maximal haemodynamic support
Investigations
Monitoring
- BGL control
- Hourly lactate
- Urine output
- Renal function
- Currently, there is no consensus on the appropriate method of invasive hemodynamic monitoring to assess and guide treatment of cardiogenic shock
Management
- Treat the lungs (effusion and pulmonary oedema):
- BiPAP or CPAP
- Consider drainage of large effusions for patients in respiratory distress
- If mechanical ventilation is used, lung-protective strategies should be implemented if feasible (e.g. tidal volume of 6-8 mL/kg of predicted body weight)
- Optimise cardiovascular haemodynamics
- Rate
- Maintain AV synchrony with pacing
- Aim for rate of 80-100 but if evidence of diastolic dysfunction or LVOTO can consider slower rates
- Rhythm
- Maintain sinus rhythm and reverse AF
- Optimise MAP
- Afterload reduction in those with high MAP/SVR
- Consider in patients with:
- HFrEF with LV dilatation
- Mitral regurgitation
- Unnecessarily high MAP (also see Acute Pulmonary Oedema)
- Can be obtained with agents such as:
- High dose nitroglycerine infusion
- Nitroprusside infusion
- Nicardipine
- Milrinone
- Consider in patients with:
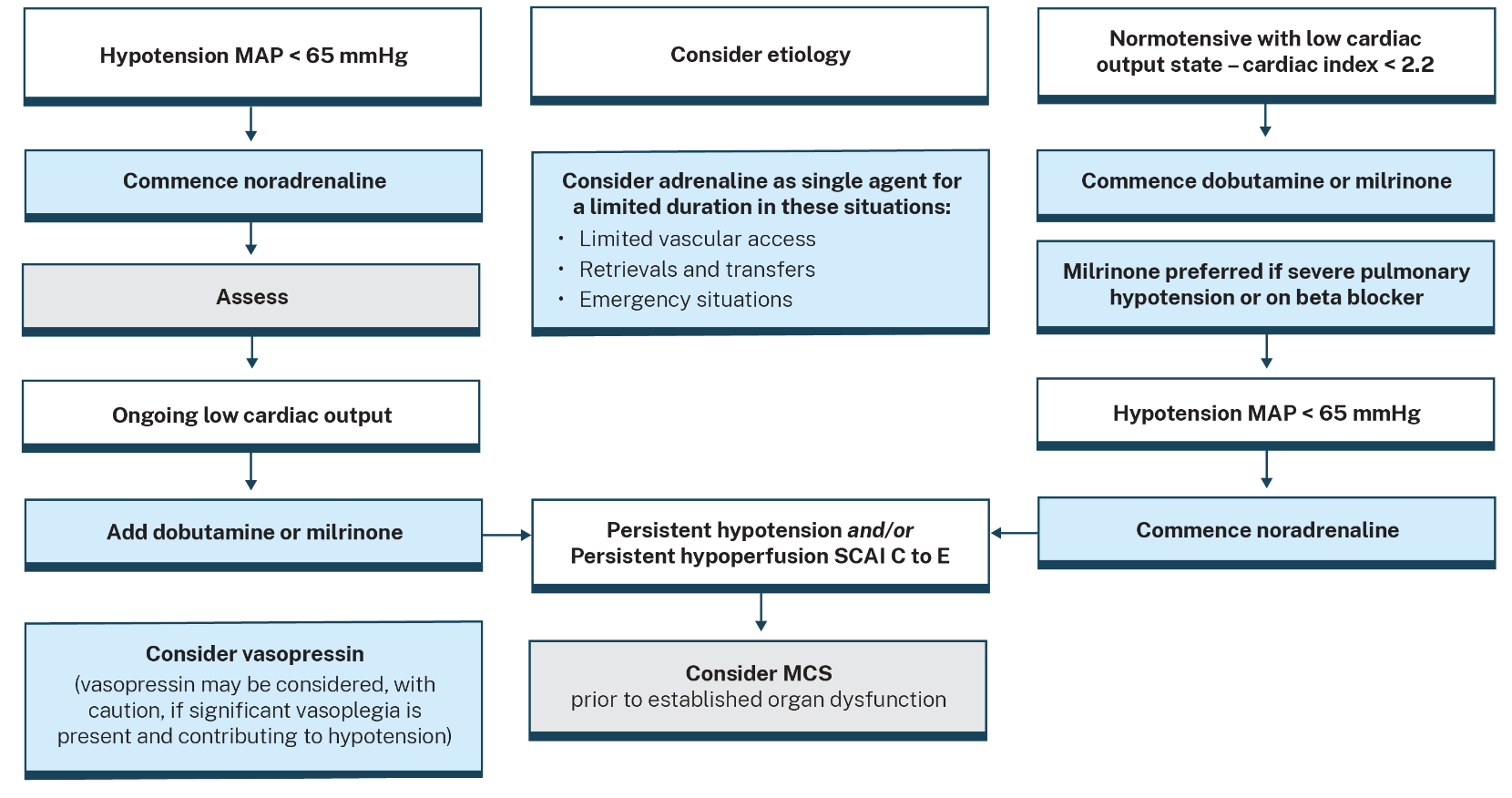
- Hypotension: consider inopressor
- Noradrenaline is widely recommended as the front-line agent for cardiogenic shock: improves SVR and elevates diastolic pressure to improve coronary perfusion
- Dobutamine or milrinone to vasodilate systemically and reduce LV afterload
- Consider pulmonary vasodilators to decrease RV afterload
- Afterload reduction in those with high MAP/SVR
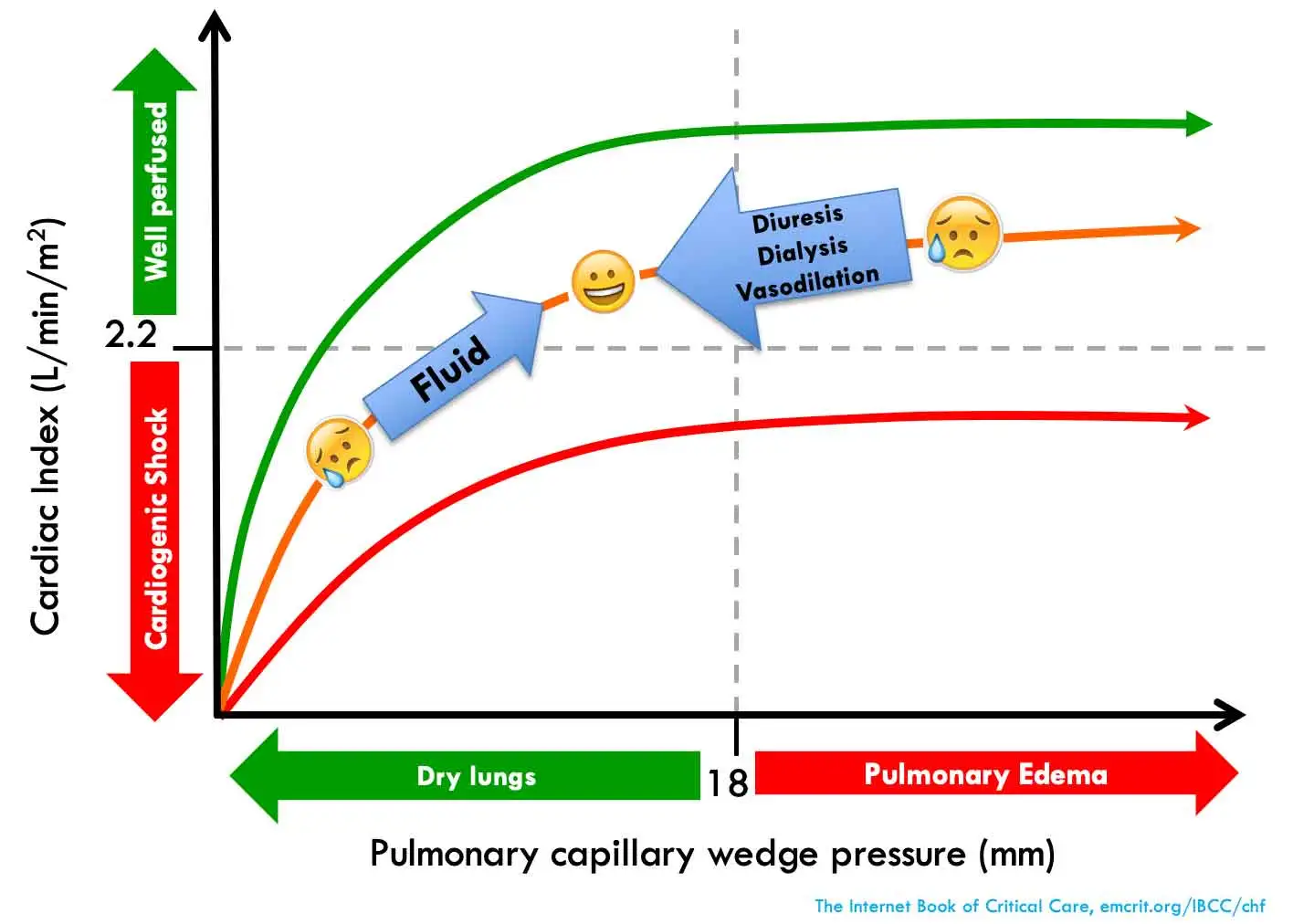
- Optimise volume status
- Fluid administration
- Give fluid when all are met
- There is insufficient end-organ perfusion (e.g., acute kidney injury)
- There is no evidence of pulmonary congestion (e.g., no B-lines on lung ultrasonography)
- The overall assessment suggests true hypovolemia (e.g., no systemic congestion)
- Dynamic indices suggest that the patient is fluid-responsive
- Give fluid when all are met
- Fluid removal
- Consider diuresis when1:
- There is significant pulmonary and/or systemic congestion (e.g., RV failure with high CVP).
- Overall assessment suggests total body fluid overload
- Clinical signs of uraemia
- Metabolic acidosis
- Refractory hyperkalaemia
- For patients who aren’t responding adequately to furosemide, consider adding a thiazide diuretic
- Consider diuresis when1:
- Fluid administration
- Rate
- Consider inotrope for low cardiac output with signs of peripheral vasoconstriction (e.g. cool mottled peripheries; knee mottling)
- Ideal first-line ionotrope is yet to be determined by RCTs
- Dobutamine appears to be commonly used and is recommended in ACI health guidelines
- Dobutamine may cause hypotension due to vasodilatory effects and should be used in combination with noradrenaline to support a MAP > 65 mmHg
- Where refractory, levosimendan and phosphodiesterase 3 inhbitors such as milrinone can be used
- Consider digoxin in patients with long-standing atrial fibrillation and systolic heart failure2
- Adrenaline is reasonable as a first line single agent in an emergency as a bridge to improved central venous access or retrieval to percutaneous intervention procedures
- Treat the underlying cause
- Arrhythmias
- ACS to be managed with revascularisation
- Anaemia
- Pericardiocentesis
- Vasopressors
- Noradrenaline is probably the vasoconstrictor of choice for hypotension and inadequate tissue perfusion
- Note the following:
- Noradrenaline and dobutamine should be first line for cardiogenic shock with mainly left ventricular dysfunction
- Noradrenaline and milrinone should be reserved for cardiogenic shock with mainly right ventricular dysfunction
- Noradrenaline and levosimendan should be considered a second-line therapy on the basis of difficult pharmacokinetics on the part of the latter, and are equally recommendable for both LV and RV dysfunction
- Adrenaline as a solo agent is recommended only for shrt-term support while waiting for expert care,
- Dopamine and vasopressin aren’t recommended for anyone
- Mechanical circulatory support devices
- Intra-Aortic Balloon Pump
- As shown by the IABP-SHOCK II Trial (Thiele H 2012) you cannot give every patient with cardiogenic shock an IABP
- IABP may be appropriate in the following cases:
- Patients with mechanical complication of AMI (e.g. acute mitral regurgitation, post-infarction VSD) where it is used as a bridge to surgery
- Temporary haemodynamic support when pharmacological therapy is failing and patient is being transferred to higher-capability centres3 (e.g. for ECMO or impella)
- Impella
- DanGer Shock Trial showed benefit in patients meeting the following criteria:
- STEMI with cardiogenic shock
- Undergoing emergency PCI
- No cardiac arrest
- No RV failure
- No significant hypoxia
- No mechanical complications
- Age under ~77 years
- Also consider in:
- Progressive/refractory cardiogenic shock SCAI stage D-E on any aetiology
- SCAI C failing medical therapy
- Non-AMI aetiologies (e.g. HF-related, myocarditis)
- High-risk PCI support
- Contraindications:
- Mechanical aortic valve
- Severe aortic regurgitation (device worsens AR)
- Severely calcified/stenotic aortic valve
- Severe peripheral arterial disease (femoral access)
- Left ventricular thrombus
- Ventricular septal defect (relative)
- DanGer Shock Trial showed benefit in patients meeting the following criteria:
- VA-ECMO
- Intra-Aortic Balloon Pump
- Heart Failure management as appropriate:
- HFrEF: SGTL2, ACE-i/ARB/ARNI, aldosterone antagonist, iron infusion, verciguat, diuretics, digoxin
- HFpEF: SGTL2, diuretics (e.g. loop, MRA, thiazide), AF management, HTN management, OSA
Sources
- Blogs
- Guidelines
- Review Articles
- Thiele H, Hassager C. Cardiogenic Shock. New England Journal of Medicine. 2025;394(1):62-77. doi:10.1056/NEJMra2312086
- Papers
- Thiele, H., Zeymer, U., Neumann, F.-J., Ferenc, M., Olbrich, H.-G., Hausleiter, J., Richardt, G., Hennersdorf, M., Empen, K., Fuernau, G., Desch, S., Eitel, I., Hambrecht, R., Fuhrmann, J., Böhm, M., Ebelt, H., Schneider, S., Schuler, G., Werdan, K., 2012. Intraaortic Balloon Support for Myocardial Infarction with Cardiogenic Shock. New England Journal of Medicine 367, 1287–1296. https://doi.org/10.1056/NEJMoa1208410
- Møller JE, Engstrøm T, Jensen LO, Eiskjær H, Mangner N, Polzin A, Schulze PC, Skurk C, Nordbeck P, Clemmensen P, Panoulas V, Zimmer S, Schäfer A, Werner N, Frydland M, Holmvang L, Kjærgaard J, Sørensen R, Lønborg J, Lindholm MG, Udesen NLJ, Junker A, Schmidt H, Terkelsen CJ, Christensen S, Christiansen EH, Linke A, Woitek FJ, Westenfeld R, Möbius-Winkler S, Wachtell K, Ravn HB, Lassen JF, Boesgaard S, Gerke O, Hassager C; DanGer Shock Investigators. Microaxial Flow Pump or Standard Care in Infarct-Related Cardiogenic Shock. N Engl J Med. 2024 Apr 18;390(15):1382-1393. doi: 10.1056/NEJMoa2312572. Epub 2024 Apr 7. PMID: 38587239.
Footnotes
-
Earlier initiation of renal replacement therapy in the absence of these conventional emergent indications has been shown to have no effect on outcome ↩
-
Patients with new-onset atrial fibrillation might benefit from cardioversion to sinus rhythym instead ↩
-
There is a NSW health policy directive on IABP and ECMO retrieval ↩