- See Shock
Overview of RUSH Exam
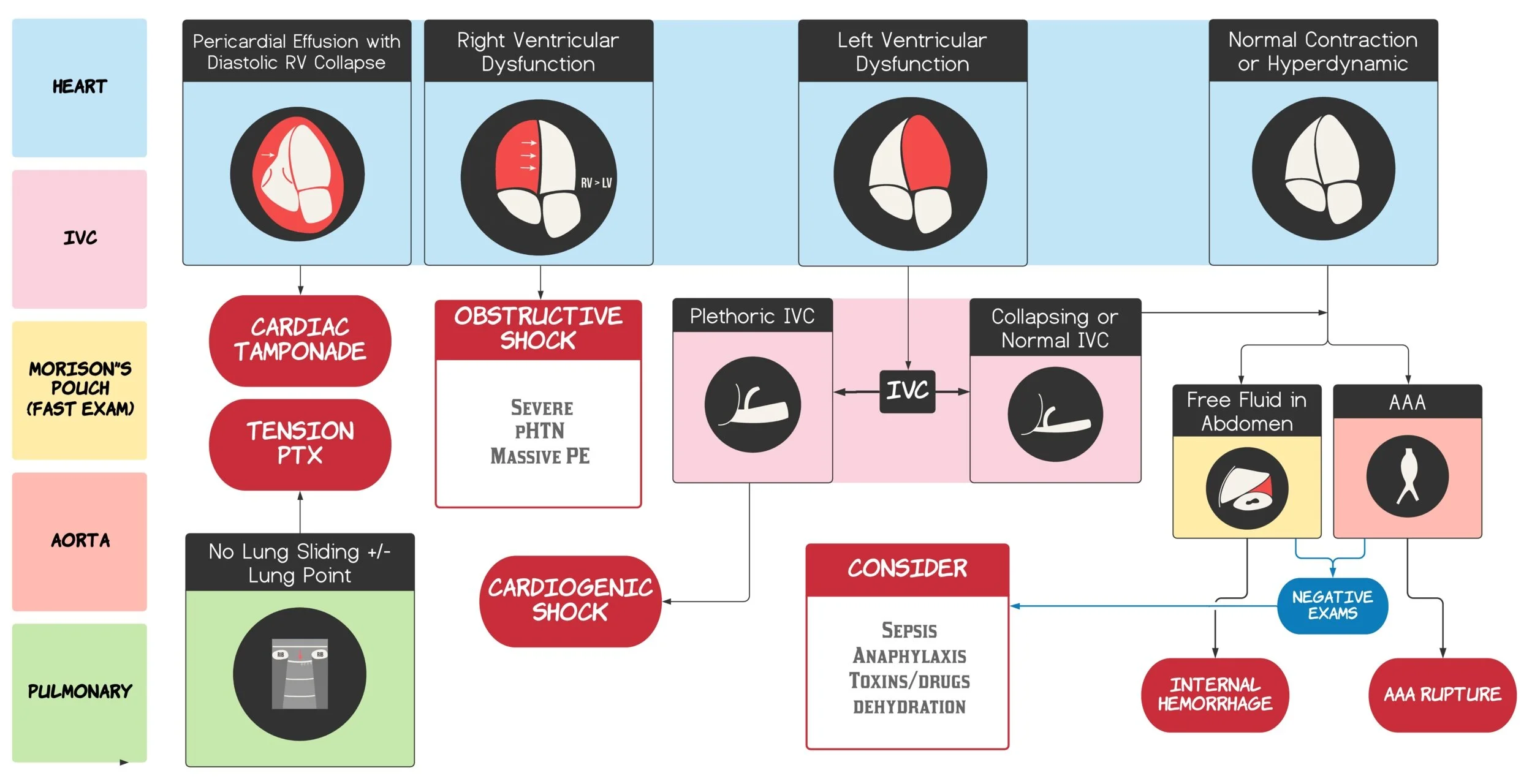
- Heart: LV function, RV dilation, pericardial effusion/tamponade
- IVC: size and collapsibility (volume responsiveness)
- Lungs: B-lines (pulmonary oedema), pneumothorax (absence of sliding)
- Abdomen: free fluid (haemoperitoneum, ruptured AAA)
- Aorta: AAA
- Lower limbs: DVT (if PE suspected)
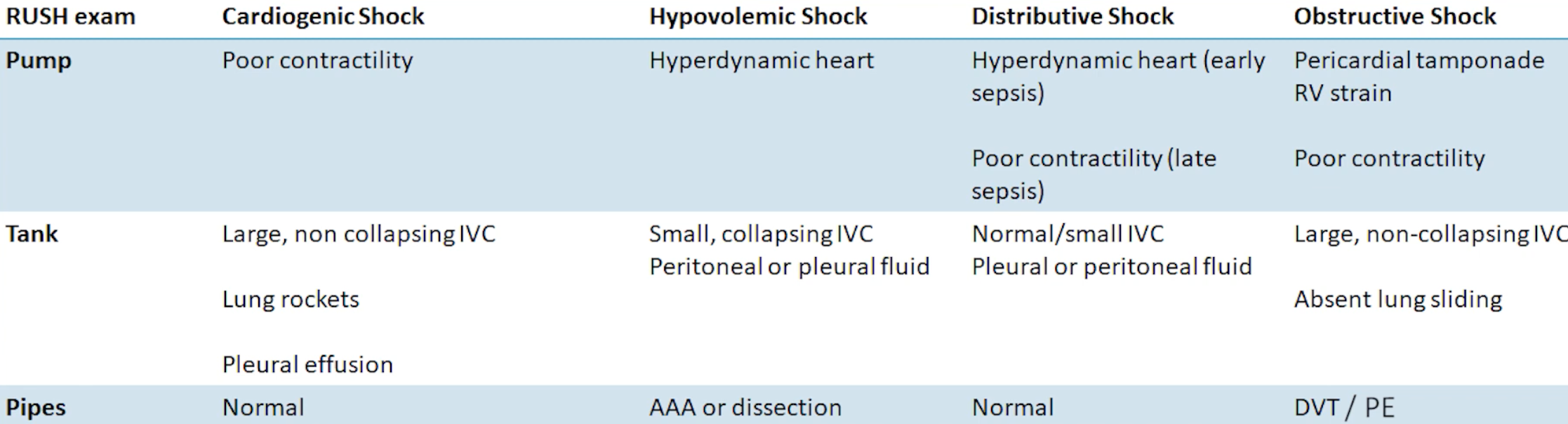
Can use the mnemonic HI-MAP (Heart, IVC, Morrison’s pouch, Aorta, Pneumothorax) or alternatively go in the approach of pump (heart), tank (IVC, Morison’s pouch), and pipes (aorta, DVT)
Heart
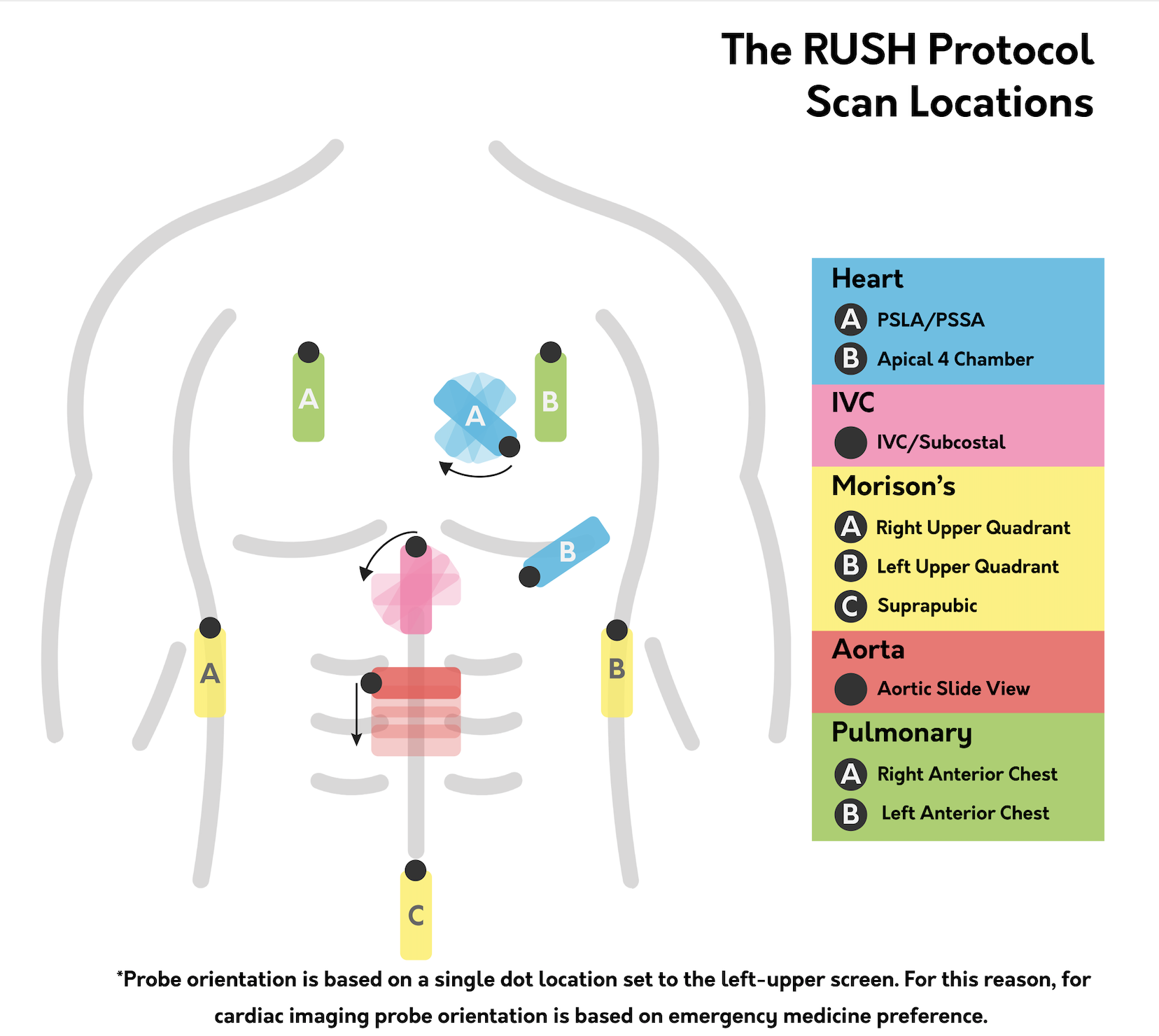
- Four standard views (PLAX, PSSA, A4C and subxiphoid)
- Assess:
- LV contractility (can be just a visual qualitative assessment)
- Example of reduced LV function
- Example of reduced LV function
- RV strain and dysfunction
- Example of RV strain with RV dilation on PLAX:
- McConnell’s sign (suggests pulmonary embolism)
- Decreased RV movement with apical sparing (apex moves normally)

- Example of RV strain with RV dilation on PLAX:
- Pericardial tamponade
- Look for a circumferential anechoic fluid collection
- Diagnostic Confirmation: Look for right ventricular end-diastolic collapse (highest specificity) or right atrial systolic collapse (highest sensitivity), paired with a plethoric IVC
- Crucial Exception: A collapsed IVC in the presence of a pericardial effusion makes tamponade highly unlikely unless severe concurrent volume depletion is present
- LV contractility (can be just a visual qualitative assessment)
IVC view
- Review the IVC in the subcostal view with the probe marker pointing towards the patient’s head
- Qualitative assessment of IVC:
- A flat IVC suggests distributive or hypovolaemic shock
- Plethoric IVC (>2 cm in maximal diameter with minimal respiratory variation) suggests right or left ventricular failure or an obstructive process or volume overload
- Collapsed (< 1.5 cm with complete/near-complete respiratory variation): Strongly points toward preload deficiency, matching hypovolemic or distributive shock states.
- Normal (1.5 to 2.0 cm with standard respiratory variation): Indeterminate; does not cleanly rule out any shock type.
- Plethoric (> 2.0 cm with minimal/no respiratory variation): Points toward obstructive aetiologies (tamponade, massive PE, tension pneumothorax) or cardiogenic failure.
- Technical Pitfalls:
- Diaphragmatic Tethering: Do not measure directly at the diaphragm, as mechanical attachment holds it artificially open. Always measure roughly 2 cm distal to the right atrial junction or just distal to the hepatic vein inflow.
- Off-Axis Narrowing: Coming off the true vessel midline makes the IVC appear artificially narrow. Switch to a transverse plane to verify the true maximal diameter.
- Aorta Confusion: Confirm identity by tracking the hepatic veins draining into the IVC or spotting the branch points of the celiac trunk and SMA on the aorta
Morrison’s Pouch
- Right upper quadrant view is most sensitive so often start at this
- Left upper qudrant view
- Supra-pubic view
Aorta
- Look in the 3cm just above the umbilicus
- If the infra-renal abdominal aorta is >3cm and the patient is hypotensive, assume it is ruptured as POCUS is not sensitive enough for retroperitoneal bleed
Pneumothorax
- Scanned using a high-frequency linear probe oriented sagittally at the anterior, least-dependent chest wall (typically 2nd to 4th intercostal spaces along the mid-clavicular line, where free air rises in a supine patient).
- Look at both anterior lung zones to observe for lung sliding (see Lung POCUS) or B-lines suggesting fluid overload
- Ruling Out Tension Pneumothorax:
- Lung Sliding: A normal shimmering, horizontal relative movement along the hypoechoic pleural line. Its presence bilaterally completely excludes a tension pneumothorax at that site.
- Comet-tail Artifacts / B-Lines: Vertical reverberation artifacts that cross the deep screen. Their presence confirms visceral and parietal pleural contact, ruling out a pneumothorax at that interspace.
- Confirming Pneumothorax:
- Absence of Lung Sliding: Highly suspicious for pneumothorax in this acute context.
- Lung Point: The exact physical junction where the visceral and parietal pleura separate due to air. Finding a lung point is 100% diagnostic of a pneumothorax.
- M-Mode Signatures:
- Seashore Sign: Normal lung. Smooth, linear horizontal lines above the pleura (the “sky”) and a granular, sandy artifact pattern beneath the pleura due to lung movement (the “beach”).
- Barcode / Stratosphere Sign: Pneumothorax. The lack of subpleural movement creates uniform, static horizontal lines tracking all the way down the screen.
Next Steps
- Once the aetiology of shock is found, to determine whether the patient’s hypotension would respond with fluids or pressors assess their Fluid Responsiveness with the LVOT VTI
Source
- RUSH: Undifferentiated Hypotension — TPA
- Youtube videos
- USS images from the pocus atlas (CC BY-NC 4.0) The Pocus Atlas